
The U.S. is widely known to have the highest health care expenditures per capita in the world, and not just by a little, but by a lot. I'm not going to go into the reasons for this so much, other than to point out that how to rein in these costs has long been the proverbial political hot potato. Any attempt to limit spending or apply evidence-based guidelines to care runs into a buzz saw of criticism.
Indeed, most of the resistance to the Patient Protection and Affordable Care Act (PPACA), otherwise known in popular parlance as "Obamacare," has been fueled by two things: (1) resistance to the mandate that everyone has to buy health insurance, and (2) the parts of the law designed to control the rise in health care costs. This later aspect of the PPACA has inspired cries of "Rationing!" and "Death panels!" Whenever science-based recommendations are made that suggest ways to decrease costs by reevaluating screening tests or decreasing various tests and interventions in situations where their use is not supported by scientific and clinical evidence, whether by the government or professional societies, you can count on its not being long before these cries go up, sometimes eve from doctors themselves in the form of Ayn Rand-worshiping libertarian doctors who think that Medicare is unconstitutional, that doctors' autonomy should be virtually unlimited, and that there should be in essence no constraints on them.
My perspective on this issue is that we already "ration" care. It's just that government-controlled single payer plans and hybrid private-public universal health care plans use different criteria to ration care than our current system does. In the case of government-run health care systems, what will and will not be reimbursed is generally chosen based on evidence, politics, and cost, while in a system like the U.S. system what will and will not be reimbursed tends to be decided by insurance companies based on evidence leavened heavily with business considerations that involve appealing to the largest number of employers (who, let's face it, are the primary customers of health insurance companies, not individuals insured by their health insurance plans). So what the debate is really about is, when boiled down to its essence, how to ration care and by how much, not whether care will be rationed. Ideally, how funding allocations are decided would be based on the best scientific and clinical evidence in a transparent fashion.
The study I'm about to discuss is anything but the best scientific evidence. In fact, to me it appears to be a political hatchet job designed to cast doubt on the very concept of any sort of government-run health care system.
A couple of weeks ago, I noticed articles and posts on blogs I follow about a study released in the April 2012 issue of Health Affairs that looked at cancer outcomes in the U.S. compared to cancer care in Europe and announced American Cancer Patients Live Longer Than Those in Europe; Higher-Priced Cancer Treatments in US Offer Better Survival:
The United States spends more on cancer care than European countries, but a new study published in Health Affairs suggests that investment also generates a greater "value" for US patients, who typically live nearly two years longer than their European counterparts.
Tomas Philipson, the Daniel Levin Chair in Public Policy at the University of Chicago, and his coauthors found that the cost of cancer treatment in the United States was higher than such care in ten European countries from 1983 to 1999. However, they also found that for most cancer types investigated, US cancer patients lived longer than their European counterparts. Cancer patients diagnosed during 1995-99, on average, lived 11.1 years after diagnosis in the United States, compared to just 9.3 years from diagnosis in Europe.
As Steve Novella put it, a single study doesn't necessarily mean anything. More importantly, this is a classic example of a study whose conclusions do not follow from its evidence and methods. So let's dig in, shall we? We'll start by taking a look at the actual study itself, which, unfortunately, is behind a paywall; so I'll try to cite as much of it as I think relevant. The article is by a group led by Tomas Philipson, the chair in public policy at the University of Chicago and is entitled An Analysis Of Whether Higher Health Care Spending In The United States Versus Europe Is 'Worth It' In The Case Of Cancer.
Here's the abstract:
The United States spends more on health care than other developed countries, but some argue that US patients do not derive sufficient benefit from this extra spending. We studied whether higher US cancer care costs, compared with those of ten European countries, were "worth it" by looking at the survival differences for cancer patients in these countries compared to the relative costs of cancer care. We found that US cancer patients experienced greater survival gains than their European counterparts; even after considering higher US costs, this investment generated $598 billion of additional value for US patients who were diagnosed with cancer between 1983 and 1999. The value of that additional survival gain was highest for prostate cancer patients ($627 billion) and breast cancer patients ($173 billion). These findings do not appear to have been driven solely by earlier diagnosis. Our study suggests that the higher-cost US system of cancer care delivery may be worth it, although further research is required to determine what specific tools or treatments are driving improved cancer survival in the United States.
Before I discuss the article, I'm going to pause here for a moment to ask you, our readers, whether you can figure out just from this abstract what the fatal flaw of this paper is most likely to be. It should be mind-numbingly obvious to longtime readers who've read some of my previous posts on cancer screening, and, in fact, the authors try to preemptively address this criticism. They fail, but they do mention it.
Now, if I were to tell you that most of the difference in survival between U.S. and European cancer patients reported in the study was driven by breast and prostate cancer, do you know what I'm trying to hint at? Sadly, health bloggers who should know better didn't pick up on this flaw. Not surprisingly, this study's findings are being touted in some circles as evidence that the U.S. does better treating cancer and, by extension, that our current system is better than any sort of government-run system.
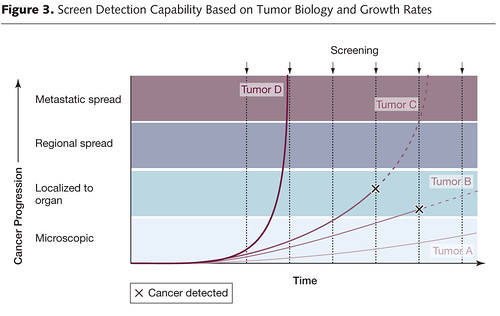
There's just one problem with this study. That problem is embodied in three words: Lead time bias. Remember lead time bias? I've written about it enough times before, particularly in the context of discussing overdiagnosis and overtreatment. Basically, using the time from diagnosis to the time of death is not the correct way to analyze data like this. To explain why, a picture is worth a thousand words (not that it'll stop me from writing a thousand words, as is my wont, because to me a picture plus a thousand words is equal to two thousand words). So here's a picture I've used before to illustrate lead time bias:

In this illustration, we see how early detection, when a cancer is in its preclinical phase (i.e., before it can be detected by symptoms or clinical examination), screening can make survival after diagnosis seem longer even if the treatments used have no effect at all. Unless the rate of progression from the point of a screen-detected abnormality to a clinically detected abnormality is known, it is thus very difficult to figure out whether a treatment of the screen-detected tumor is actually improving survival when compared to tumors detected later. If investigators are to do so, the lead time needs to be known and subtracted from the group with the test-based diagnoses. Moreover, this lead time is usually stochastic. It will be different for different patients, with some progressing rapidly and some progressing slowly. This variability, as I have discussed before, is responsible for a second type of bias, known as length bias, which is illustrated thusly:
Basically, what this graph illustrates is how screening programs preferentially pick up tumors that are growing slowly and more likely to portend a good prognosis (or represent overdiagnosis), rather than tumors that are rapidly growing and likely to portend a worse prognosis. This problem is at the heart of the issue of overdiagnosis. Basically, overdiagnosis, as I've discussed before, refers to disease detected by a screening test that, even if not treated, would never threaten the life or seriously threaten the quality of life of a patient. In the case of cancer, for instance, I've pointed out how frequently such disease is found in autopsy specimens. For instance, although the prevalence of clinically apparent prostate cancer in men aged 60 to 70 was only around 1% 20 years ago, at the time it was known that 40% of men in their 40s have histologic evidence of the disease. Thyroid cancer has a prevalence of around 0.1% of clinically apparent disease in adults aged 50 to 70, but autopsy studies looking at thyroids very finely find at least one papillary thyroid cancer in at 36% of adults. As I've pointed out elsewhere before as well, if breast tissue is looked at closely enough in an autopsy series of women between 40 and 50, foci of breast cancer can be found 39% of the time. In other words, aggressive screening can lead to more patients having a diagnosis of cancer for a longer period of time even without any real improvement in survival.
What all this means is that looking at population-level survival rates as a surrogate for how well a country is doing against cancer is fraught with confounders, in particular lead time bias. In a country where there is a lot of screening for cancer (hellooo; the United States!), lead time bias will be a bigger issue. There will also be more overdiagnosis, which will inflate the apparent survival time after a cancer diagnosis in the population. In such a case, we would anticipate that some of the largest gains in apparent survival would be in cancers for which major screening programs were undertaken, cancers like breast and prostate cancer, which is exactly what the authors observed. Now consider the time period that the authors chose to examine: 1983 to 1999. That is exactly the time period when large screening programs for breast and prostate cancer were being implemented, both in the U.S. and Europe. For example, in the U.S., breast cancer screening has traditionally been much more aggressive: Every year instead of every two to three years, as is common in many European countries and Canada, and beginning at age 40 rather than age 50, which is why these two graphs from the paper are not at all surprising. Here's "Exhibit 1." I have no idea why it's called that instead of "Figure 1," but it's annoying and perhaps emblematic of how such a paper could have been accepted for publication in the first place. It's as though the Philipson et al view their paper as a set of legal, rather than scientific, arguments:

Notice in the first one how the survival rate curves are almost perfectly parallel. This sort of a graph is exactly what I would expect if lead time bias were largely responsible for the difference in survival between the European Union and the U.S. Sure, that might not be the entire explanation, but seeing a graph like this sends up huge red flags, as does this figure:

This latter "exhibit" suggests that the vast majority of the detected survival advantage in the U.S. was due mainly to breast and prostate cancer, exactly the two cancers for which screening programs were ramped up beginning in the late 1970s through the 1980s.
Given the common knowledge of how lead time bias affects comparisons of the sort Philipson et al did, I really wanted to know why Philipson et al chose to look at survival statistics from time of diagnosis, rather than cancer death rates or another measurement:
The term survival gains refers to increases in years of life expectancy from cancer diagnosis seen over time. We decided to focus on examining survival gains over time because doing so provides insight into the progress that countries have made relative to their own baselines. An analysis that focuses instead on levels of survival is more likely to be influenced by intrinsic population characteristics, such as genetic predisposition to cancer, and might not reflect the impact of different health care systems.
This, of course, utterly misses the point of why looking at survival as a surrogate, at least aggregate survival rates for cancer, is generally easily confounded by lead time bias and other factors, in particular overdiagnosis. That's why mortality rates are a better measure for how well we are doing against cancer. They aren't affected by lead time bias, overdiagnosis, or length bias. One of the best explanations of why mortality rates are a better measure on a population level for how we are doing against cancer than survival rates was provided by Aaron Carroll:
Let's say there's a new cancer of the thumb killing people. From the time the first cancer cell appears, you have nine years to live, with chemo. From the time you can feel a lump, you have four years to live, with chemo. Let's say we have no way to detect the disease until you feel a lump. The five year survival rate for this cancer is about 0, because within five years of detection, everyone dies, even on therapy.
Now I invent a new scanner that can detect thumb cancer when only one cell is there. Because it's the United States, we invest heavily in those scanners. Early detection is everything, right? We have protests and lawsuits and now everyone is getting scanned like crazy. Not only that, but people are getting chemo earlier and earlier for the cancer. Sure, the side effects are terrible, but we want to live.
We made no improvements to the treatment. Everyone is still dying four years after they feel the lump. But since we are making the diagnosis five years earlier, our five year survival rate is now approaching 100%! Everyone is living nine years with the disease. Meanwhile, in England, they say that the scanner doesn't extend life and won't pay for it. Rationing! That's why their five year survival rate is still 0%.
None of this is to say that screening for cancer is useless. I've never said that, nor do I believe it. I have, however, explained that demonstrating real increases in survival due to screening is devilishly difficult, far more difficult than "common sense" would lead the average person (or even physician) unschooled in the intricacies involved would think, hence the controversy over prostate and breast cancer screening and, in particular the UPSTF recommendations from two and a half years ago regarding screening mammography.
Aaron Carroll also did me a favor and saved me a lot of work by compiling mortality rates for various cancers in G8 countries as another way to illustrate what is almost certainly closer to the real situation. The fact that he did it for years much more recent than the time period Philipson et al. did was rather curious, of course, but maybe not so much so given that more recent statistics show that most European countries have results much closer to those in the U.S. than 20 years ago. Be that as it may, Carroll points out that the U.S. is among the best in the world when it comes to breast cancer but not actually the best. Japan appears to be doing much better than the U.S. As a cancer surgeon, I will point out that breast cancer in Japan might be different, possibly due to lifestyle differences. In terms of other cancers, Carroll concludes that for cervical cancer, we're in the middle of the pack; for colorectal cancer, we're unequivocally doing the best; and for prostate cancer we're in the high end of the middle of the pack. The most interesting observation is that for lung cancer we are doing abysmally. The obvious excuse for that is tobacco smoking, but it turns out that the U.S. has one of the lowest rates of tobacco use of these countries; so that doesn't explain it. As Aaron's last cancer graph shows graph when it comes to overall mortality from cancer, compared to the G8 countries, the U.S. is doing well but is not the best. As Aaron sums it up:
Not nearly where you'd like to see us. Because we don't do as well with some of the more prevalent cancers, we wind up doing much worse overall when it comes to cancer mortality than you'd think. This is why, when some point to us having the "best" health care system, they focus on colon cancer or breast cancer, not on lung cancer. Overall, though, we're not.
I can't help but notice, too, that if you really want to compare countries with universal health care systems to the U.S. (and, let's face it, that's what this is really all about, trying to show that "socialized medicine" leads to "death panels," health care rationing, and lower survival rates for deadly diseases like cancer), you really should include Japan in the mix. The problem, of course, is that Japan does a lot better than the U.S. in many areas. My point, however, is not to denigrate the U.S. healthcare system. It does quite well in some areas, not so well in others, and overall it's very good but not spectacular, at least when we look at cancer mortality. The real problem is not that the U.S. system doesn't deliver quality cancer care. Rather, the problem is that delivering that care in the U.S. is spectacularly expensive for the results it gets compared to other countries that spend considerably less.
Surprisingly (to me at least), there's been some really good reporting that punctures the claims of this particular study. First, there's this one, in which Steven Reinberg interviews Dr. Otis Brawley, the chief medical officer and executive vice president at the American Cancer Society. Dr. Brawley points out that, yes, overdiagnosis is likely the fatal confounder not accounted for by Philipson et al.
More impressive is Reuters article by Sharon Begley, in which she explains very well why this study doesn't show what Philipson et al conclude that it shows. Also, unlike the case in some other posts and articles that I've seen dealing with this study, Begley doesn't suggest that Philipson et al completely ignored lead time bias. In all fairness, before finishing, I have to state unequivocally they didn't. The problem with their analysis is that they made a highly unconvincing argument using mortality statistics for why they don't think lead time bias was a major confounder of their results. In fact, they did some rather amazing contortions to try to justify their approach of focusing on survival statistics instead of mortality rates, even to the point that they included an online supplement in which they examined mortality rates in the various countries included in their study. Here's the problem with that argument, which is summed up very well in Begley's article:
The Philipson team acknowledges that survival data can be misleading. They justify their approach, however, by saying that because deaths from cancer as a percentage of a country's population fell faster in the United States than in 10 countries in Europe from 1982 to 2005, the higher U.S. survival "suggests that lead-time bias did not confound our results."
Some experts in cancer statistics were not convinced.
"Why do the authors use the wrong metric - survival - in the analysis and then argue that the right measure - mortality - provides corroborating evidence?" asked Welch. "As long as your calculation is based on survival gains, it is fundamentally misleading."
Indeed. I found that very curious myself, particularly how the justification was buried in an online supplement, rather than described in the text of the paper itself. It makes me wonder if it was something the authors cooked up to justify themselves after peer reviewers started hammering them on the issue of lead time bias. It wouldn't surprise me in the least if that were the case, although, again in all fairness, it might not be. Similarly, their lame argument that they chose increases in survival as their metric because it would allow them to compare each country to its baseline made me laugh. Do they seriously believe that following mortality trends over time wouldn't allow them to compare each country to its baseline? Is it just me? Am I alone in finding such an argument ... unconvincing?
In reality, there are two ways to study how well different countries are doing in terms of cancer care. One way is, as mentioned several times in this post, to focus on cancer mortality. Another way is much more difficult in that it involves comparing stage-specific survival rates, and, for cancers for which there are screening programs, survival rates for screen-detected cancers and survival rates for all cancers. The latter is an analysis that is very difficult to carry out, given that not all countries have good registries that have cases properly stratified by stage and that it wouldn't be able to compare how countries are doing against all cancers overall, only individual cancers. Also, stage definitions change over time, and carrying out such an analysis would involve taking such changes into account--not an easy adjustment. Yet, Philipson et al. chose to do neither of these things; indeed, they picked the very metric for which confounding factors, such as lead time bias and overdiagnosis, tend to be the most problematic.
I wonder why. Actually, I don't, at least not anymore, considering the author's affiliation with the American Enterprise Institute and Manhattan Institutes, think tanks which routinely engage in denial of science like global warming. As I said before, this is not a scientific paper. It's a policy paper designed to smear anything that has even a hint of the dreaded "socialized medicine" about it.
More importantly, I wonder how this study ever passed peer review. One would think that Health Affairs would have at its disposal a cancer epidemiologist who understands overdiagnosis, lead time bias, and length bias to tap as a peer reviewer. I guess not. Heck, I'm more than willing to make myself available the next time a right wing think tank tries to publish something this bad. I'm not even a biostatistician, and I could see the enormous flaws in this turkey.
Maybe US costs are so high because policy is so heavily affected by profit-lobbying, more so than in Japan or the UK?
40% of 40 year old men have detectable prostate cancer? I heard that sitting on a tennis ball can help? Has anyone tried getting a large number of men to sit on a tennis ball for 90 to 600 seconds each day? Is there a significant gain? or is a study needed?
AEI and Manhattan Institutes, oh my!!
You missed Philipson's fellowship with the Heartland Institute whose dedicated climate change denial work and determined efforts to defend smokers' rights so endears it to the public. Heartland goes so far,at least in the climate change denial field, to pay a number of so-called "scientists" to write truthy scientific papers.
http://www.desmogblog.com/heartland-institute-exposed-internal-document…
With a lead author with affiliations like that I'd have to suspect woo research until proven otherwise and Exhibit 1 does look wonky.
The problems you so neatly demonstrate concerning lead time bias are also prevalent in my own specialty area of infectious diseases.
In the early days of the AIDS epidemic when (barely effective) treatments were also being used, the literature abounded with useless studies about improved "survival", with few people taking into account the issue of earlier HIV screening and lead time biases.
Another significant bias entered affected analysis of HIV survival within defined populations infected roughly around the same time point - that of the rapid progressors dying earlier, and the ones who were naturally slower progressors surviving longer. This was a major confounder when trying to tease out how real the benefits of HIV therapy were in those individuals (the ones getting the latest drugs being the ones who were the naturally slower progressors, with the historical comparator "controls" actually being those who were intrinsically more rapid progressors).
So how do the approximately 50 million US residents without health insurance fare when compared to residents of 'socialist' European countries who get government subsidized basic health care? As someone of Hungarian ancestry I might add that 50 million is approximately 10x the population of Hungary... seems like an awful lot of disposable people living in the US of A, eh?
Studies such as the one reported here make me wonder whether the authors are deluding themselves with their ideological biases, or whether they're intentionally being disingenuous.
['Disingenuous' is such a useful euphemism.]
Have you an article on the advisability of 10yr colonoscopy screenings for over 50? (I'm discussing this with my doctor).
In the UK, if you have no family history of colon or rectal cancer, they'll give you 3 fecal occult blood tests (samples taken one day apart) every 2-3yrs. If any are positive, then they recommend a full colonoscopy. In addition, they recommend a one time flexible sigmoidoscopy for those 55 - 65.
This seems to be a better (and more comfortable!) screening procedure. Your thoughts?
I have mentioned here before that when I was working in a UK NHS hospital lab measuring PSA a few years ago we only considered PSA to be clinically indicated if the patient was over 40 and had symptoms of prostatitis. I used to go through the request forms to weed out those that didn't fit the criteria and would send out a report explaining why we would not do the test. I'm pretty sure that is the usual policy in the UK, which would result in later and fewer diagnoses and a reduced lead time here.
I know that at least one regular commenter here had his life saved by routine PSA screening. I admit to feeling a little uncomfortable knowing that if that PSA request had landed on my desk I would have refused to do it, which would have had grave consequences.
On the other hand, you have to consider the effects of overtreatment for prostate cancer, which can also have grave consequences. As Orac says, screening is complicated and can have all sorts of counterintuitive effects.
I'm so tired of hearing single payer health care systems like those in the UK and Canada demonized as "socialized medicine!" While their governments underwrite the cost of their citizens health care, the health providers themselves aren't government employees but independent contractors.
If this is "socialized medicine", Boston's Big Dig highway project was "socialized construction".
Anyway, between Medicare, Medicaid, and the tax break for employer-provided insurance, the government already pays for a huge chunk of it.
Let's see here: Of $598M in total benefits for all kinds of cancer, $627M is for prostate cancer and $173M is for breast cancer. Which, if I'm adding correctly, leaves -$202M for all other kinds of cancer combined. Where were the referees thinking when they let that statement pass?
Even before you mentioned Philipson's AEI affiliation, I was suspicious of his motivations. The University of Chicago is home to a school of economics notorious for constructing elegant economic theories which utterly fail to explain economic data, and insisting on the correctness of their theories when it is pointed out that they do not explain the data. I call it Lysenkoist economics, because it would be rather convenient for certain powerful people if that school of economics were true, and it's difficult for junior economics faculty in many departments to oppose this school. While Philipson's title leaves it ambiguous whether he himself is an economist, it's certainly plausible (especially considering his other affiliations), and most of his co-authors seem to be economists.
Oops: the amounts I quoted from the abstract should be billions, not millions. So the problem is a thousand times worse than I indicated.
This study from 2008 from Lancet Oncology comes largely to the same conclusions that the above study does - namely that there does seem to be an advantage in the US for these cancers (though interestingly Cuba wins in breast cancer).
Cancer survival in five continents: a worldwide population-based study (CONCORD)
http://www.lancet.com/journals/lancet/article/PIIS1470-2045(08)70179-7/…
This study seems to have less lead-time bias, since they look at " ï¬rst, primary, malignant, invasive neoplasm ", so it seems to be more stage-specific, though your judgment is obviously better than mine here. It was also performed by a collection of European hospitals, not a US right-wing think tank.
Thomas @11 -- Very interesting.
I'm sure the idea of Cuba "winning" in any kind of measurement would send many on the right into paroxysms of blind rage, because in their world that kind of thing simply is not supposed to happen.
Global warming can't be happening, either, because stopping it would require some kind of collective action, of which Ayn Rand would surely have disapproved.
It's always interesting how often Ayn Rand comes up in these discussions, especially knowing she died of lung cancer but only after quietly using the Medicare she espoused against to pay for her treatment.
A powerful takedown of Rand can be found here.
It's interesting how often the phrase "Follow the money," seems to be spot on. Once you know the affiliations (and therefore presumably the paymasters) of the authors of this "study", suddenly the conclusions make more sense.
My take-away from Aaron Carroll's graphs is that the poor beleagured NHS has its work cut out. More a result of under funding than anything else, I'd imagine, and will only get worse with the austerity measures being put into place.
#13: "espoused against" I'm not sure "espoused" means what you think it does.
I find entirely too many Rand lovers in too many topics. Sometime I should do a blog post on her, but the horror stories I hear about her writing make me reluctant to slog through the firsthand sources.
This appears to be house style for article components that are "editable" (see author instructions, 8b). It's a clumsy name, but not apparently intrinsic to any particular paper. In fact, having figures that are "smart" enough to cough up their data if requested, assuming that's part of the idea, is a good thing.
Using "exhibit" in place of "figure" is apparently standard practise in some areas of economics and finance theory.
Its use in this context should raise red flags, as it indicates that the authors are economists rather than professionals in any relevant specialty.
- Jake
Yup, Wharton School with a postdoc at Chicago, which he hasn't left, although the specific affiliations have jumped around.
Overseas they have cheap drugs that are not FDA approved here in the good old USA. My overseas acquaintances are doing much better than the US medians for our latest and greatest medicines, for cents on the US treatment dollar.
Please tell me that Obamacare is going to deliver more cost effective medicines and diagnostics by simply catching up with the rest of the world, not just denials by rationing.
To me, funding, overdiagnosis and overtreatment aren't the largest problems. Rather it's simple protectionism and price gouging, often 10, 20, 30 fold costs per element of treatment or diagnosis.
About lead author Tomas Philipson: he is one of three partners at Precision Health Economics. The other two partners in this private company, (Darius Lakdawalla and Dana P. Goldman) are two of the five co-authors of this study. Michael Eber who is the second listed author is listed as a team member/consultant at Precision Health Economics, as well.
http://www.precisionhealtheconomics.com/team
Here's another analysis of this report which discusses the affiliations of the authors with conservative think tanks and conflicts of interests of some of the authors:
http://pnhp.org/blog/2012/04/11/is-higher-u-s-health-care-spending-on-c…
The last three paragraphs are especially interesting about the authors past affiliations and present conflicts of interest.
Orac, you're going to make me cry. You don't read my articles anymore?
Uh, didn't I link to your post not just once but twice? :-)
Oh wait, now I see it. Sorry.
Anyway, we should write the HA editors and suggest they find new jobs for letting this tripe through and lose whatever reviewers put a pass on this garbage. One of your jobs as an editor of a journal isn't just wrangling reviewers and looking for typos, it's making sure bad science doesn't contaminate the literature. This shouldn't have even passed triage.
Of course those oversea drugs are approved by the European equivalent of the FDA, the EMEA (and having interacted with both I assure you the EMEA standards for approval are as higher or in some respects higher than the FDA's.)
And we could achieve a similar reduction in cost, if we were in a position to take advantage of free-rider pricing and embraced a single payer system as does much of the rest of the world. (Of course there is the question of who would we free ride with--ourselves?)
"My perspective on this issue is that we already "ration" care. It's just that government-controlled single payer plans and hybrid private-public universal health care plans use different criteria to ration care than our current system does."
This is a false definition of "rationing". Rationing means allowing access to only a fixed amount of something. By virtue of being able to buy healthcare with money, it is, by definition, not rationed.
What is rationed in the USA is the supply of new doctors, wherein the number of intern and residency positions are controlled via a government sanctioned monopoly.
Of course, the USA does suffer from overdiagnosis and overtreatment, as this study rightly points out, but providing more screening and more price-insensitive care to more people will only exacerbate this situation. It is far better to move insurance to catastrophic care, where it belongs. Employer provided health care coverage in the US isn't so much insurance as a tax avoidance scheme.
Hello USA. You are being lied to by rich people. Figure out who the loudmouths in your media are and shut them up once and for all. They are warping the way you perceive the world around you. Once you have done that, grab everyone that is afraid of socialism and reeducate them so they realise that the public sector and private enterprise can work in harmony, that there is nothing to be afraid of and that they themselves are holding back your economic recovery.
According to this blog...the study was partially funded by Bristol Myers-Squibb, a major manufacturer of cancer drugs. Was this fact disclosed in the full article?
http://reforminghealth.org/2012/04/11/is-the-high-cost-of-cancer-care-r…
Fred the Hun - usually I don't comment on tone, but frankly your use of the phrase "disposable people" got on my nerves. It appears intended to demonize people. What about those who believe people should pay for their own medical services, but contribute to charitable medical foundations? Or those who believe there are higher priorities for government spending, but help out their relatives?
static vars--
By that logic, the UK isn't rationing care either, because patients have the option to "go private" for things that the NHS won't cover, or that it will cover but only with a longer wait than the patient is comfortable with.
Other than by broad health outcomes (years of wellness, disease prevalence, age at mortality etc)How is it possible to make any reasoned comparison of national healthcare systems when one of those systems excludes from treatment the most health challenged 17% of its population ? It's painfully obvious that poorer people have worse recovery rates and experience faster decline across all illnesses. If one healthcare system is dependent upon exclusion of the most challenging patients (even if only in pre-retirement), and another is intrinsically stuctured to include all patients, what commonality of metric can apply ?
Mephistopheles @30 (cc: Ben the Hun). At the risk of sounding simplistic, the problem is that medical care for acute conditions is so catastrophically expensive that a great many people simply can't afford it, so that we have two choices: (a) ensure that society somehow provides a reasonable standard of medical care to everyone when they need it, through some scheme or other; or (b) watch people die.
Hence the phrase "disposable people" for the uninsured. It's rhetorically powerful, but I think fair -- a whole lot fairer than "death panels", which were basically assembled out of the whole cloth.
"My perspective on this issue is that we already "ration" care. It's just that government-controlled single payer plans and hybrid private-public universal health care plans use different criteria to ration care than our current system does."
It's my longstanding observation that "horror stories" about the US private system and European "socialized" system tend to share a common element: a bueaucratic holdup in preventive or "quality of life" care. Thus, I'm inclined toward the opinion that the whole debate over private v. state-sponsored medicine just distracts from even more fundamental issues.
David N. Brown
Mesa, Arizona
Care to share, or are you satisfied sitting in the corner pretending to be profound?
Could be that US is doing bad in the lung cancer because there are more poor smokers than rich?
It would be interesting to have the mortality data for EU and US divided by income.
Another possible source of confusion is that in "socialized" health-care countries probably all cancers are detected, maybe in the US poorest people die even before being diagnosed.
richard77 @36 -- That's a very interesting point.
The smoking rate in the US is EXTREMELY correlated with social class. In my part of the world (New England), it seems as if the whole working class smokes, and none of the upper middle class smokes, with the exception of a few artsy-type kids.
Palindrom - by that standard, pedestrians are disposable people as well.
Mephistopheles @38
"Palindrom - by that standard, pedestrians are disposable people as well.
Perhaps I need a second cup of coffee this morning... would you care to flesh that analogy out a bit for me?
Dammit, I've got some data on this-really I do-but it's under embargo until the EHA meeting for one bit and until the journal gets through fussing with it for the other. For right now, I'm simply going to make the bald, unbacked assertion that it's not that simple. At least not for lymphomas. There are interesting differences which simply won't be seen if one looks at overall cancer survival or even overall survival for a specific cancer. Including age and other characteristics reveal differences not obvious in the overall measure.
This study showed a mixed picture when survival in Germany and the US were directly compared. It's probably not even that simple though, for a couple of reasons. First, the US data is almost always derived from SEER. The SEER database is wonderful, quite complete, etc. However, there is at least one study which suggests that survival in the SEER dataset is higher than in the US in general. So modest differences might disappear if a truly equal comparison was made. Conversely, HIV rates are higher in the US so some of the differences seen may be due to HIV rather than treatment in the respective countries.
Sure - pedestrians share the same roadways with vehicles weighing thousands of pounds and travelling tens of miles per hour. If a pedestrian is hit by a motor vehicle (and many are) they stand a chance to be killed. The fact that we as a society do not provide pedestrians with protection against vehicles (say, steel barriers to prevent vehicles from hitting pedestrians, or policeman at every corner to enforce safety rules, or impact resistant cages to move around in) suggests that we're standing idly by and consider these people to be disposable.
Mephistopheles @38 --
Just to be clear, the term "disposable people" is not meant to suggest that these peoples' lives SHOULD be valued any less than any other person's life. It is meant to convey moral indignation at the way in which some classes of people are treated as if there lives WERE less valuable than those of others.
And by that standard, pedestrians are, in many circumstances, also disposable, in just the same sense that the uninsured are. In New York City (as the wonderful blogger BikeSnobNYC reminds us frequently), motor vehicles reap a terrible harvest of pedestrian and bicyclist lives, and the police seldom seem to hold the drivers responsible, or give the cases any kind of priority. The same holds in many other jurisdictions as well.
Is that helpful?
Along the same lines, we know how to produce buildings that will withstand tornadoes - at least in the form of safe rooms and storm shelters. Yet we have no program to provide these for those who can't afford them. Are people without safe rooms or storm shelters in tornado prone areas disposable people?
palindrom,
I got the point of the comment entirely. My objection to it is that I don't believe it is accurate in these cases.
You can make a very good case that someone considers a certain group to be disposable if they, say, force them to cross a mine field in order to be sure it's safe.
Not paying for all their health care, not so strong a case in my view.
Mephistopheles O'Brien @ 42
Actually, we do have grant funding for safe rooms and storm shelters in various forms.
http://www.fema.gov/plan/prevent/saferoom/funding.shtm
Mephistopheles O'Brien @ 42
Actually, we do have grant funding for safe rooms and storm shelters in various forms.
http://www.fema.gov/plan/prevent/saferoom/funding.shtm
Mephistopheles@ 43
"Not paying for all their health care, not so strong a case in my view."
My point has to do more with providing basic primary care to everyone.
I happen to be a dual US/Brazilian citizen so I have firsthand knowledge of the what happens there as well. I was just down in Brazil recently and had the opportunity to discuss health care with a cousin of mine who holds a Masters degree in health sciences and is the head nurse at a large hospital in Sao Paulo. She also volunteers her time to provide health care to former residents of a shantytown who have been relocated to government provided housing. It seems that even though Brazil has a long way to go at least they are on the right track!
"Healthcare in Brazil is provided by both private and government institutions. The Minister for Health and Ageing administers national health policy. Primary health care remains the responsibility of the federal government, elements of which (such as the operation of hospitals) are overseen by individual states. Public health care is provided to all Brazilian permanent residents and foreigners in Brazilian territory, and is free at the point of need (being paid for from general taxation)"
Source Wikipedia
This policy of providing care for the less privileged sectors of Brazilian society in no way impedes anyone with the means`to do so, to pay for private or specialized care but it does guarantee that everyone has access to basic primary care at no cost if necessary.
The long term benefits to Brazilian society as a whole seem to far outweigh the costs.
We in this country, seem to be unable to grasp this simple concept for some strange reason.
Mephistopheles @43 -- Then we simply disagree. As a citizen of a major industrialized country, I am more than willing to bear a tax rate high enough to ensure reasonable standard of health care to all citizens. If it were administered intelligently -- which is a stretch given the interest groups influencing policy -- it wouldn't even be ruinously expensive, and would probably be substantially less of an overall burden than we bear now.
jaquesk - I stand corrected with regard to people who live in pre-manufactured homes.
@35,
As I intended to indicate in the initial comment, I am inclined to view the central "problem" as the involvement of bureaucracy. Admittedly, that's not an observation that's going to be very helpful in solving anything, the it might be useful to state as a central question: "How do we make bureaucrats responsive to doctors more than vice versa?"
@Fred the Hun,
You offer a reasonable observation, but the fairest conclusion to draw from it is simply that the US and Europe are so different that ANY venture at comparison is necessarily tenuous.
Under the present system, we all *pay* for care for the uninsured. The only difference is that the uninsured do not have access to a *medical home* for preventive care and for interventions for cancer and other serious medical conditions.
Consequently, when uninsured people arrive in the hospital, it takes a large chunk of our scarce medical care tax dollars to treat them or to cure them. The human costs for uninsured people who arrive at hospitals with late stages of cancers that are now incurable, is a sad commentary about a segment of our society who believe that some people are not worthy to have the good medical care that insured people have.
I am not pleased that the issue of a National Health Care Plan has resulted in the watered down legislation that was passed by Congress. Nor am I pleased with the Medicare Part D coverage that was passed during the Bush administration, that did not include a provision to negotiate the price of commonly prescribed drugs. (This legislation had wide support from drug manufacturers):
http://www.ncpssm.org/pdf/price_negotiation_part_d.pdf
We would have a golden opportunity here, to really change our system from a private medical insurance system to a universal health care system, yet we still cling to our antiquated and splintered funding streams for health care, that excludes a huge segment of society who are uninsured. Sad.
Mephistopheles @49:
Actually, it's not limited to manufactured homes (otherwise known as trailers). Read further down. The info at that link needs a little updating but it's mostly accurate.
I work with the latter two programs mentioned--HMGP and the soon-defunct PDM--on a daily basis. Those programs can and do provide funding for wind mitigation projects, including general wind-resistant construction (saves costs by reducing structural damage) and saferooms (tornado shelters). Public and private structures are eligible, such as schools and homes. With very limited exceptions for special projects such as education and outreach, all projects must pass benefit-cost analysis, and applications are reviewed for eligibility and quality. The selection of projects depends on State priorities and local interest as they are ultimately grants to local jurisdictions.
Overall I'd say hazard mitigation is underfunded and undersupported at all levels, Fed, State and local. Especially considering its net long-term fiscal benefit. Nonetheless, HMGP and PDM have a solid track record in most states and have done well in mitigating the cost and hardship of natural disasters.
@48 palindrome
I do live in an industrialized country (alright, it's New Zealand so 'industrialised' is probably a bit strong, but we're a first world country even if we do have more cows and more sheep than people) and I do bear a tax rate high enough to ensure reasonable standard of health care to all citizens. And it is awesome. We have a mixed public/private system so there are private hospitals available for people who can pay, and public hospitals for people who can't. I see a private GP because I can afford it, but I could never have afforded to go private for my recent ovarian surgery, so that was done in the public hospital. In the waiting room for my pre-surgery ob/gyn check was a refugee who was having some problems with her female circumscion. I don't mind paying an extra percent (and the amount more that I pay compared to an American earning the same money is really very small) to ensure that she gets good treatment too.
jaranath,
I didn't read that in your link, but clearly you know. I have a cousin who came out of her neighbor's storm cellar to find the entire neighborhood gone (not trailers), so I expect she'll be interested. Thanks very much.
No problem, happy to help. She would need to speak to her local government about the possibility of applying, as the actual applicant must be the local jurisdiction (city, county, etc), and they apply to the State, who decides on what projects to pursue. Projects covering multiple homes have better chances than single homes (nearly the same amount of work to run a project with ten homes vs. one). Given the aforementioned funding and support issues, there's a decent chance she wouldn't be able to get funds, but the State and FEMA also have some guides available for how to build saferooms, and there are a lot of not-outrageously-priced commercial prefab or in-ground options. Shades of the 1950s...I think some of them are even the same designs! :)
@51,
The cost of the "uninsured" in the US needn't be limited to medical care. In all likelihood, not having insurance is just a "symptom" of some other problem, the most obvious being that the person is in the country illegally. That's an issue that I think makes it especially hazardous to compare the US medical system with anything in Europe: The closest analog to the US illegal and/or Latino population in Europe would be Arabs and Muslims, but even they generally a) come from countries with a fairly high standard of literacy and economic development and b)don't come in on foot!
@56
One third of the population of Alabama under the age of 65 are uninsured. But only 3.9% of the population are Latino (and that includes people there leagally).
The highest estimated number of illegals in the US is 20 million. And that figuire is very suspect. The number of uninsured people in America is 50 million.
Look, I love a good 'it's the illegals' answer myself. It makes things so much simpler because the problem is 'them'. But I don't think the numbers stack up in this case.
It's also worth noting that illegal immigrants can drive from the East to the EU. Or walk, if they prefer. I know they're not Muslim or Arab so maybe they don't count?
@56
One third of the population of Alabama under the age of 65 are uninsured. But only 3.9% of the population are Latino (and that includes people there leagally).
The highest estimated number of illegals in the US is 20 million. And that figuire is very suspect. The number of uninsured people in America is 50 million.
Look, I love a good 'it's the illegals' answer myself. It makes things so much simpler because the problem is 'them'. But I don't think the numbers stack up in this case.
It's also worth noting that illegal immigrants can drive from the East to the EU. Or walk, if they prefer. I know they're not Muslim or Arab so maybe they don't count?
@papango,
I said that being in the US illegally is the "most obvious" reason somebody would be without insurance, nothing about it being the only one. As far as that goes, it isn't just illegals who might fear repercussions if they put themselves on the grid by applying for health insurance. An example in my own back yard would be the polygamist colonies in northern AZ.
As for your scenario of driving into the EU, what you're talking about is, strictly speaking, going from eastern Europe to central and western Europe. I can't regard that kind of traffic (which DOES include Muslims) as comparable to immigration of Arab and/or North African Muslims.
@59
Seriously? Are Arabs and African Muslims really that different from Albanians? or Kazakhs? or Kurds or Turks? And that those places are economically developed. That seems a little flimsy. Is it that Albanians can simply drive in Greece, rather than walk? And Mexico has a higher literacy rate than any North African country. Your distinction is more than a little arbitrary.
I'm leaving this now, because I know from painfully experience that in the US immigration has layers of overtones I don't see from out here in the Pacific.
David N. Brown @ 59
"I said that being in the US illegally is the "most obvious" reason somebody would be without insurance, nothing about it being the only one."
No, that simply isn't true!
http://www.usatoday.com/news/nation/2010-09-17-uninsured17_ST_N.htm
The reasons for the rise to 50.7 million, or 16.7%, from 46.3 million uninsured, or 15.4%, were many: workers losing their jobs in the recession, companies dropping employee health insurance benefits, families going without coverage to cut costs. Driving much of the increase, however, was the rising cost of medical care; a Kaiser Family Foundation report shows workers now pay 47% more than they did in 2005 for family health coverage, while employers pay 20% more.
Those 50 million people they are talking about are not here illegally, they just can no longer afford the price of admission.
" I am inclined to view the central "problem" as the involvement of bureaucracy."
The costs of bureaucracy, or the less pejorative 'administration' is one of the reasons why state run health payment systems are so much more efficient than private. We have a deeply ludicrous mixed system in Australia. People who buy private insurance are subsidised by huge tax rebates. And the private funds have at least 3 times the administration costs of the public system.
So instead of employing a few administrators for state controlled salaries, the tax system pays for bloated bureaucracies in 'private' health funds, with little to no say in how these places are run or how they decide their own salaries. At least the mixed system in the UK is strictly public or strictly private. Not public or generously taxpayer subsidised private like ours. Madness.
What about Norway, Sweden, Denmark, Iceland, Finland, Luxembourg, Switzerland, Austria, Belgium and The Netherlands - countries were health care really is socialized. Has these countries been compared to the US?
The CIA World Factbook is your friend.
Here are % of GDP spent on health figures. Note that only Malta spends more than the USA. Australia, UK, Canada and most European countries spend less than 10%.
https://www.cia.gov/library/publications/the-world-factbook/rankorder/2…
Use the search box at the top to look for life expectancy and other health criteria. (I didn't want to disappear into moderation by putting in all those links.) There are some surprises there.
@Fred Magyar,
I think I've failed to make a crucial point clear: Presumably, anyone who doesn't buy health insurance is economically disadvantaged. But the economically disadvantaged are characteristically at further disadvantages: recent immigrants, established racial/ethnic minorities, isolated subpopulations, the disabled, etc, etc. It can logically be expected that these groups are being particularly hard-hit by the recession, by any measure. (Indeed, there are some indications of a trend, in cases as disparate as the FLDS in Arizona and the Amish out east, of people from characteristically isolated and distrustful subpopulations coming out of the woodwork to seek healthcare.) On the other hand, it wouldn't be unduly surprising if the historically disadvanted have actually fared better (comparatively!) than the "mainstream" population.
@adelady,
Something I think comes with the involvement of a bureaucratic infrastructure is that getting care becomes dependent on specific diagnoses rather than self-evident need. Private and public systems both seem to lend themselves to this problem, as insurance companies pick and choose what to pay for as a matter of self-interest while government agencies can waste years just deciding whether to recognize a condition. This was pretty much the situation for me and others who grew up with Asperger's Syndrome before psychiatrists got around to recognize it.
"...while government agencies can waste years just deciding whether to recognize a condition."
Not sure what you're getting at here. In Australia, the amounts paid as government rebates for consultations and procedures are calculated on various criteria, but the decisions about diagnosis and need for treatment are decided by the professionals involved.
The only bureaucratic "interference" is in identifying over-servicing and fraud. We no longer have any GPs wandering through the local nursing home after dressing Mrs Wotsis' leg ulcer, waving at everyone s/he knows and claiming rebates for 40 consultations for half an hour's work. A few did that, got stomped on, nobody does it now.
There are issues about deciding which drugs do and don't get subsidised on the Pharmaceutical Benefits Scheme. But once again, there's no direct involvement in professional decision-making about 'recognising' conditions. Unless you talk about off-label prescriptions, which are not eligible for subsidy because it's not in accordance with the approval schedule. It's the professional associations which advance the scientific assessments to justify extending the 'label' applicability to more conditions.
Most of the subsidy arguments nowadays are about extraordinarily expensive new drugs, usually for cancer treatment, which threaten to eat the whole budget for generic insulin or other vital, life-saving, treatment-saving drugs. Or new improved versions of existing drugs which the subsidy scheme considers offer too little benefit for the much larger costs the pharmaceutical companies want to charge.
In spite of my expressed desire to have a national health care plan, there are many "scams" that are prevalent using the Medicare (permanently disabled and/or 65 years of age) and Medicaid (indigent) health care plans.
It happened here in nursing homes, in much the same way as "adelady" describes it. Recently, a small nursing home owner/doctor was found to be in cahoots with an ophthalmologist. The in-house doctor was sending every resident out for day surgery for cataract removal/intra-ocular lens implants. The two doctors ended up billing Medicare and Medicaid for millions of dollars, for unnecessary surgeries...and ended up with criminally charges of battery.
I recently saw a documentary on television showing *strike teams* that are raiding clinics and durable medical equipment suppliers. The teams were heavily armed, as some of the operators of the clinics/medical suppliers have criminal records.
About two years ago, I received a statement from Medicare and among the actual physician visits was an *odd* bill from a Florida psychologist for a pre-admission evaluation to an inpatient psychiatric facility. I immediately called the Medicare telephone number, explained that I don't live in Florida and had not seen this doctor and instructed them to investigate immediately, lest the cost of the inpatient psychiatric treatment be billed under my name. It turns out that the bill was submitted under a different name for a person with a Florida address; the only thing that tied this patient to me, was an inadvertent wrong social security/Medicare number, which is mine. I also alerted my secondary private health care provider to deny payment, should they receive any more bills associated with care in Florida.
I still am upset that this bill was not questioned by Medicare because it had the wrong name, wrong address, and wrong date of birth.
I have a great private drug plan, that *encourages* the prescribing of generic drugs, in lieu of branded drugs. The cost of a generic drug is $ 5/3 months supply, rather than $ 50 for the same 3 months supply. There are exceptions made for anti-convulsant drugs, when used exclusively for seizure control...not as psychiatric drugs, whereby brand names are dispensed and billed to the policyholder at the generic prices.
A friend who is on expensive chemotherapeutic drugs for multiple myeloma has the same drug plan as I have. There is a *cancer center of excellence* specifically set up within that drug insurance company. I imagine that this proves to be a very efficient manner to have highly trained case managers to make decisions about these very expensive drugs.
"I have a great private drug plan, that *encourages* the prescribing of generic drugs..."
Our national PBS does something similar. Every time we fill a prescription, the pharmacy assistant asks if we'll accept a cheaper substitute if one's available. We always say yes. If you say no, the user pays a higher fee - unless the doc has gained pre-approval for a specific named version of the drug for a patient with particular medical indications.
@ adelady: My drug insurance plan also *encourages* mail-away pharmacy services. If you fill "maintenance type" of drugs (for hypertension, cardiac drugs, etc) at the local pharmacy, the co-pays are higher for the generic and brand name drugs.
I have computer access to my drug plan. The company actually emails "reminders" to me, for renewal of maintenance drugs every three months. The written doctors prescription is *good* for a year's supply (4 separate orders/90 days supply).
I renew maintenance drugs on-line and the drug plan mails the drugs to me and also bills my VISA charge card, because I provided my account number to the plan...eliminates writing a mailing a check.
For one-time prescriptions (antibiotics, eye drops, etc.), I go to the local pharmacy, where my drug plan and my subscriber ID number are available through the pharmacy computer.
Has anyone ever looked into Medicare Part D...the drug prescription plan that Medicare recipients buy into? This plan was advanced by the Bush II administration. While it is helpful for Medicare recipients, it is a billion dollar yearly boondoggle because it does not include "negotiating" prices for drugs with drug manufacturers. Negotiating for prices is what the Veteran's Administration and other government agencies do, to stretch taxpayer dollars and Bush II wanted the *support* of *Big Pharma*.
I consider myself quite savvy when it comes to reading and interpreting insurance coverages contracts, but this Plan D has me totally flummoxed with its provisions, including the notorious "donut hole":
http://en.wikipedia.org/wiki/Medicare_Part_D_coverage_gap
Note also that the Obama health care plan, which is being reviewed by the USSC for constitutionality of its provisions, would have revised the Plan D Medicare Coverage to simplify it and to provide better coverage with less cost to Medicare subscribers.
@adelady,
The kind of problem I'm talking about is that even those in obvious need may be refused services simply on the grounds that the pros can't put a label (or the "right" label) on what's wrong with them. I don't know about the rest of the world, but it CAN and I have no doubt does happen in the US. Really, it's not only a problem for our healthcare system; it's also a major issue in the school system.
Something else I feel bears on this is the occasional mutterings about parents trying to get a child diagnosed with autism just to get welfare and/or other benefits. I strongly suspect that such things do happen, except, I think the most likely motive would not be greed, but a lack of recognition and services for another diagnosis or none.
David N. Brown
Mesa, Arizona