
It should come as a surprise to no one that I'm not exactly a fan of "integrative oncology"—or integrative medicine, or "complementary and alternative medicine" (CAM), or whatever its proponents want to call it these days. After all, I've spent nearly ten years writing this blog and nearly seven years running another blog dedicated to promoting the scientific basis of medicine, and just this year managed to publish a lengthy commentary in a high impact journal criticizing the very concept of integrative oncology. Unfortunately, it seems to be the equivalent of the proverbial pissing in the ocean, as the flood of CAM quackademic medicine continues unabated. So it was just before the Thanksgiving holiday, when I learned from the director of the National Center for Complementary and Alternative Medicine (NCCAM), Dr. Josephine Briggs, that the Journal of the National Cancer Institute had published an issue consisting of nothing but a monograph on the evidence base for "integrative oncology."
I had to take a look.
Unfortunately, there are too many articles in this monograph to cover them all in this post. In particular, there were a couple of clinical trials that demonstrate quite aptly the problems with integrative oncology as a concept. Perhaps, if nothing else grabs my attention, I will take a look at them later this week. In the meantime, what I really wanted to concentrate on what was clearly intended as the centerpiece of this monograph, a set of clinical guidelines by Heather Greenlee, Lynda G. Balneaves, Linda E. Carlson, Misha Cohen, Gary Deng, Dawn Hershman, Matthew Mumber, Jane Perlmutter, Dugald Seely, Ananda Sen, Suzanna M. Zick, Debu Tripathy, for the Society for Integrative Oncology Guidelines Working Group entitled Clinical Practice Guidelines on the Use of Integrative Therapies as Supportive Care in Patients Treated for Breast Cancer. This is, after all, where the "rubber hits the road," so to speak, in which the SIO ranks integrative oncology interventions based on what its guidelines working group considers to be the best existing evidence. The results, it turns out, are not surprising to someone rooted in science-based medicine. I'll show you what I mean.
First of all, let's look at how the guidelines were developed. First, SIO started with a working group, an expert panel, if you will, made up of members possessing expertise in medical oncology, radiation oncology, nursing, psychology, naturopathic medicine, traditional Chinese medicine, acupuncture, epidemiology, biostatistics, and patient advocacy. One wonders where the homeopaths and reiki masters were, although certainly naturopathy encompasses at least homeopathy, given how integral homeopathy is to naturopathy. In particular, one wonders why there doesn't appear to be a chiropractor on the panel, given the popularity of chiropractic, which is at least as "respectable" as naturopathy or traditional Chinese medicine and has the added advantage that some musculoskeletal manipulation might actually provide some relief for low back pain. (Read Sam Homola's excellent posts to learn what chiropractic, stripped of its vitalism, might be able to accomplish when strictly limited to musculoskeletal pain such as low back pain.) As I like to say, chiropractors are undertrained physical therapists with delusions of grandeur, but they are popular, and there's no reason I can see for the SIO to leave them off the panel, at least not compared with TCM practitioners and naturopaths, as they did actually do a search for chiropractic, as shown in the supplemental data. (Spoiler alert: None of the chiropractic modalities were found to have sufficient evidence to make a recommendation.)
It is, however, telling to look at the list of excluded modalities:
Several interventions were excluded for the following reasons. Some have already been well summarized by other groups [eg, diet (22,23), physical activity (22–24)], while others already have a large evidence-base and are often no longer included in the definition of integrative or complementary interventions as they have become mainstream [eg, cognitive-behavioral therapy (25), psychoeducation (26), counseling (27), and support groups (26)]. Others were in early or pilot stages of research (eg, attention restoration therapy) or were not considered integrative interventions for the purposes of these guidelines (eg, prayer, spirituality).
Of course, once again I must emphasize that diet and physical activity were never "alternative" or "integrative," nor was cognitive-behavioral therapy, counseling, or support groups, although all of these were oversold as improving cancer survival, as our occasional guest blogger James Coyne has described. As for the rest, prayer and spirituality are religion, not science. Overall, this list of excluded therapies is perfect as an illustration of the arbitrariness and falseness and of the very concept of "integrative medicine," as is the manner in which the SIO defined these therapies itself:
Complementary and alternative therapies are generally defined as any medical system, practice, or product that is not part of conventional medical care (13,14). Examples include natural products (ie, vitamins, minerals, botanicals, and fish oil) and mind–body practices (ie, yoga, meditation, acupuncture, and massage). Complementary medicine is the use of a therapy in conjunction with conventional medicine (14). Alternative medicine is the use of a therapy in place of conventional medicine. Integrative medicine is the use of evidence-based complementary practices in coordination with evidence-based conventional care. Integrative oncology refers to the use of complementary and integrative therapies in collaboration with conventional oncology care.
Again, natural products are part of conventional medical care. For instance, digoxin is derived from the foxglove plant, although, as I like to say, there is a reason we don't recommend that patients with heart failure or arrhythmias don't chew foxglove leaves to treat their heart condition. In terms of oncology, Taxol is derived from a substance in the bark of the Pacific Yew, and many chemotherapy agents were derived from natural products or the modification of natural products. The difference between using the "integrative oncology" version of natural products and the SBM version of natural products is that the "integrative" versions are crude, impure, and vary in activity from lot to lot.
Arbitrary and artificial definitions aside, the panel did an extensive literature search of nine databases (EMBASE, MEDLINE, PubMed, CINAHL, PsychINFO, Web of Science, SCOPUS, AMED, and Acutrial) from January 1, 1990 and December 31, 2013 and identified 4,900 articles, of which 203 were eligible for analysis because they were randomized controlled clinical trials of CAM interventions in breast cancer that met the inclusion criteria. It then ranked the interventions the Jadad scoring scale and a modified scale adapted from the Delphi scoring scale to result in a score from A to I defined as follows (click to embiggen):
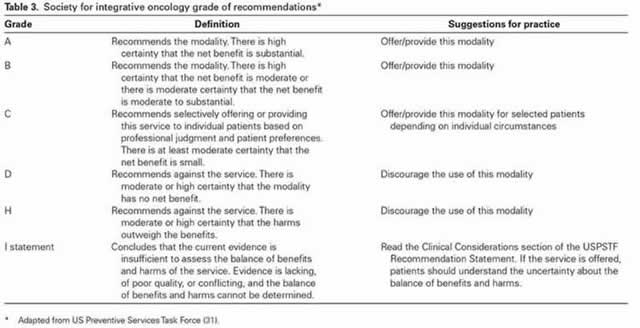
So what did the SIO find? Let's put it this way. The results were most definitely...underwhelming. For example, the only grade A recommendations were for meditation, yoga, and relaxation with imagery for routine use for common conditions, including anxiety and mood disorders (Grade A). Notice that there are no grade A recommendations for anything having to do with pain, but only for symptoms with an even heavier subjective component, namely anxiety and mood. Of course, yoga is a form of exercise and therefore nothing out of the realm of conventional medicine, given the number of studies that have shown the benefits of exercise in cancer patients. Similarly, the only grade B recommendations included stress management, yoga, massage, music therapy, energy conservation, and meditation for stress reduction, anxiety, depression, fatigue, and quality of life. Interestingly, again, none of these, with the possible exception of meditation, can be considered in any way "alternative," thus once again demonstrating how integrative oncology specifically and integrative medicine in general have co-opted treatments that should be considered conventional as somehow "alternative>" As for music therapy, massage, and the like, these represent modalities that I like to point to as examples of what we used to call supportive care that have been "medicalized" by CAM and turned into therapies when in reality they're just activities and modalities that help patients feel a bit better or help pass the time, no specific effects intended. As for massage, it is rather disappointing that SIO lumped it together with "healing touch," given that healing touch is a form of energy healing very much like reiki and thus total quackery, whereas massage at least has the benefit of feeling good to most patients.
As for the rest, surprisingly (given that this is an SIO document) but not surprisingly to anyone rooted in SBM, acupuncture does not appear as a modality in grade A or B, meaning that, at best, the SIO considers acupuncture for anything to be only worth recommending "selectively offering or providing this service to individual patients based on professional judgment and patient preferences" and deems that there "is at least moderate certainty that the net benefit is small." Electroacupuncture (which is in reality TENS rebranded as acupuncture and acupressure are given a grade B recommendation for nausea and vomiting, but that's about the best, and as I've discussed before that evidence is a bit shaky.
The key observation was that the "majority of intervention/modality combinations (n = 138) did not have sufficient evidence to form specific recommendations (Grade I)." (Grade I means insufficient evidence.) I note that the supplemental document shows that homeopathy is one of those modalities, even though there is more than enough evidence on basic science considerations alone coupled with clinical trials that show no benefit above placebo to state that it is ineffective for basically everything. Ditto reflexology, which gets a grade I recommendation for most things, but a grade C recommendation for "improving quality of life among BC patients." Meanwhile healing touch is given a grade C recommendation for "improving mood in BC patients undergoing chemotherapy." Once again, healing touch is energy medicine quackery, much like reiki. In other words, little, if anything, in these clinical guidelines gives support for real "alternative" treatments, although they do give mild support for a few potentially science-based modalities rebranded as CAM/"integrative oncology."
Amusingly, however, these new guidelines are much weaker in their recommendations than a previous set of SIO guidelines discussed by Kimball Atwood six years ago. Particularly notable is how far down the ladder of recommendation strength acupuncture has fallen since then, and the SIO, at least for breast cancer survivors, no longer recommends considering consulting a "qualified expert in CAM modality, such as an Doctor of Naturopathy (ND) who is board certified in naturopathic oncology, may be considered" when conventional therapies fail, but I'm actually not sure the SIO did this, because these guidelines are for cancer survivors. Either way, it would seem as though the more studies are examined and performed, the weaker SIO's recommendations become, which is not surprising given that most "integrative" oncology modalities are placebo.
Of course, the real reason for this monograph is not so much a critical analysis of integrative oncology, although some of the authors do appear to try to do this. The real purpose is to use an ostensibly critical analysis buying into the false dichotomy of "integrative oncology" in order to rebrand potentially science-based modalities as "alternative" or "integrative" and to provide ammunition for advocates of "integrative oncology" to start "integrating" quackery with science-based medicine. As Benjamin Kligler and Margaret Chesney state in their article in the monograph entitled Academic Health Centers and the Growth of Integrative Medicine, referring to the Consortium of Academic Health Centers for Integrative Medicine (which I've discussed before many times, for example, here and here):
Many barriers—including reimbursement challenges—still exist in the effort to make integrative approaches available as part of routine care. With the publication of this monograph though, we take an important step in removing one of the barriers to integration: the availability of high-quality research evidence on the appropriate role of integrative medicine in cancer care. We are proud to be part of this effort and look forward to the many ways in which the Consortium can provide support and momentum for researchers and clinicians in oncology as we move forward.
Except that this monograph doesn't really do anything of the sort. If anything, it confuses matters. Unfortunately, integrative oncologists have been far too successful in promoting this false dichotomy listed in the same article unironically:
The Consortium of Academic Health Centers for Integrative Medicine—an organization comprised of 57 academic health centers and health systems in North America—defines integrative medicine as follows:
Integrative Medicine is the practice of medicine that reaffirms the importance of the relationship between practitioner and patient, focuses on the whole person, is informed by evidence, and makes use of all appropriate therapeutic approaches, healthcare professionals and disciplines to achieve optimal health and healing.
As this definition implies, although an openness to using therapies such as acupuncture or massage is a component of the integrative approach, integrative medicine goes far beyond simply combining the therapies previously described as “complementary/alternative medicine” with conventional care. It describes a change in philosophy, which expands our role beyond that of treating disease to reaffirm the commitment to treating the whole person. Almost more than anywhere else in medicine, the practice of oncology and the work of caring for a patient with cancer and their family clearly call for this approach and for a commitment to whole-person care. Lifestyle counseling, behavioral medicine interventions, and spiritual support all play critical roles in this integrative approach, alongside the use of other therapeutic strategies rooted in a rigorous evidence-based approach to the best conventional care. This is integrative medicine for cancer.
No, it is a false dichotomy. It is not necessary to "integrate" quackery like healing touch, naturopathy, or acupuncture with science-based conventional medicine in order to "reaffirm the commitment to treating the whole person" or expand a practitioner's role "beyond that of treating disease." A favorite saying of mine might be a bit of a cliche, but that's OK. It's a cliche that's true. There is no such thing as "alternative," "complementary," or "integrative" medicine, nor should there be. Such medicine that is shown to be safe and effective scientifically ceases to be "alternative," "complementary," or "integrative" and becomes just medicine, and that is how it should be. Treatments that are truly effective and safe do not need the training wheels of a title like "alternative," "complementary," or "integrative." They will stand on their own to scientific testing, no special protection required, and they shouldn't be used until they have. Remember, as well meaning and sincere as its practitioners and champions are, "integrative oncology" is a Trojan horse that is depositing quackery right into the heart of academic medicine.
others already have a large evidence-base and are often no longer included in the definition of integrative or complementary interventions as they have become mainstream
I believe this is called "letting the cat out of the bag". Formerly "alternative" techniques which develop enough evidence of efficacy are adopted by science- and evidence-based practitioners, as they should be, leaving the alt-med crowd to push modalities which lack such evidence. Which tells me that the authors of this paper aren't pushing woo out of ignorance--they actually do know better. That makes them more evil than the alt-med people who push that stuff out of ignorance.
"Lifestyle counseling, behavioral medicine interventions, and spiritual support all play critical roles in this integrative approach, alongside the use of other therapeutic strategies rooted in a rigorous evidence-based approach to the best conventional care. This is integrative medicine for cancer."
I agree with this... up to a point. It is important to provide as much support as possible for a patient with cancer, but there are many, many components of supportive care that have absolutely nothing to do with medicine and shouldn't be presented as such, which "integrative medicine" does.
I especially hate when alties represent psychotherapeutic measures, relaxation and stress control as being ways to treat the cancer itself rather than as ways to assist the patient emotionally and socially.
-btw- it's International AIDS Day.
Once again CAM practitioners are guilty of thinking it is so because they wish it to be so.
@Denise,
Promoting all those psychotherapeutic modes as cancer treatment also lets those large hospitals off the hook for all the other patients with chronic illness that they do not support.
Wouldn't it be great if "integrative care" meant having a real person who co-ordinated the primary and specialty care, support services like physical therapy and social work, as well as financial counseling and the billing department?
The patient could just get treatment and get well, instead of becoming a full time administrator and clerk.
and I forgot to include the lab. work and the pharmacy.
"Integrative Oncology" is... for finding the area under what curve?
mho #5:
BINGO! A billion likes!
Really, why don't sbm advocates see people turn to CAM because the adminstration and allocation of SBM has become so damn awful under the dictates of insurance companies?
Denice #3:
I really hate it when sbmies imply that only the cancer (or whatever) itself needs to be treated, as if serious diseases somehow don't almost always have psychological consequences that manifest in part as physical symptoms that can and should be addressed by diet, exercise, relaxation, etc. etc.
Everybody:
I wonder why no one on a supposed Skeptic forum has noted the logical fallacy inherent in Orac's position.
@ sadmar:
No no no!
EVERY illness has psychological consequences; the idea to which I object is when alties insist that dealing with conflict and stress alone will CURE the cancer or whatever.
Unresolved conflicts and hidden emotions lead to cancer and serious illness.
@sadmar - the notion that people need to be supported, psychologically and physically, through serious illnesses like Cancer, is old hat.....what these people are talking about it trying to raise those support mechanisms to the level of "treatment" on par with surgery and other actual treatments of the diseases.....
sadmar:
A thousand agrees on the insurance thing.
I'm thinking fallacy of equivocation. Is that what you're thinking?
Lawrence: Old hat, yes, but that doesn't mean that we do a good job of it, necessarily.
@JTS - actually, I do agree with you. We could be doing a much better job in assisting patients, but not at the expense of legitimizing quackery.
"Integrative medicine" then looks like one of Daniel Dennett's "deepities" -- it can be true but trivial or extraordinary but false with just the flip of a mental button. You can "integrate" the science-based medical treatments with science-based lifestyle counseling and support. Or ... you can "integrate" science-based treatments with outright quackery.
Which is it? Either one or both of them, back and forth -- whatever it takes to get the other person to nod along and agree that SBM alone is limited. The advantage of using deepities is this very flexibility.
jts #14
I'm thinking a formal fallacy, but i can't figure out what it might be called.
Some examples of group G exhibit property P.
Property P has moral value MV.
Therefore, group G has moral value MV. (Leading to call to categorical action A.)
It's the same form as the au currant Dawkins/Harris fallacy:
Some Muslims engage in actions X, Y, Z, etc.
X, Y, Z, etc. are morally abhorent.
Therefore, Islam is morally abhorent. (So we should kill all the towelheads before they kill us, or something...)
Denice #10
I know alties are saying what you're saying they're saying, and anyone saying "that dealing with conflict and stress alone will CURE the cancer or whatever" is a dangerous idiot. And by echoing your wording I was not suggesting you were claiming or impying anything but.
I was perhaps clumsily attempting to suggest: 1) That legit medical insitutions indeed "could be doing a much better job in assisting patients". 2) That failure to do well enough has opened the door for quackery. 3) Thus 'doing better' is a necessary element in fighting quackery. 4) Thus 'doing better' is something sbmers need to to a better job talking about, and well, doing something about, maybe. (BTW, I'm trying to use the lowercase 'sbm' to distinguish the practice of 'science based medicine' from the blog 'Science Based Medicine'.)
Sastra #15
We can agree with Orac that there should only be 'medicine' as that term should cover whatever treatments are "shown to be safe and effective scientifically." But attempts to enforce prescriptive lexicography are a fools errand. Orac can no more wipe away the fact that a terminological distinction now exists between 'medicine' and 'integrative medicine' than I can get the internet to stop the neo-logic use of "trope". As you note, though, 'integrative medicine' does not have a fixed meaning. However, "you can 'integrate' the science-based medical treatments with science-based lifestyle counseling and support" is anything but trivial.
What SHOULD be happening (imho) is sbm should be fighting like hell to define 'integrative medicine' in a way that excludes woo — or, in marketing terms, steal the f***ing brand from the competition. That means accepting the fact on the ground that the terminological distinction between 'medicine' and 'integrative medicine' would not exist if medical institutions were indeed doing an effective job of using "science-based lifestyle counseling and support" to 'treat the whole person.' (E.g. the invocations folks get to eat better, stop smoking, get some exercise etc. at the end of their appointments with their PCPs don't actually help them to eat better, stop smoking, get some exercise etc.) Sbm ought to own up that it's institutions have dropped the ball on things science has proved are beneficial and show it is committed to fixing the damn problem. NOTHING in the quote cited in #15 justifies acupuncture, reiki, or any other woo crapola, nor does it suggest that dealing with lifestyle issues alone cures any disease. If anything, it asserts the opposite.
I submit the statement "The practice of oncology and the work of caring for patients with cancer and their families calls for a commitment to whole-person care, in which lifestyle counseling, behavioral medicine interventions, and spiritual support all play critical roles" is entirely valid. And if people are going to call that 'integrative', well, it is what it is. The philosophy itself doesn't seem to be a problem, so we're b**ching about terminology that is not going to go away.
The term is fuzzy exactly because it arises from legitimate discontent with institutionalized medical practice, articulating a desire for change, but not at all settled on what changes would be appropriate and what would be inappropriate. If it gets de-fuzzed to include quackery, that would be very bad. But just because quacks are making a claim for the term, and trying to use it to ride the coattails of legitimate reform into legitimacy doesn't mean that's going to happen. Heck, the quacks have been claiming 'medicine' forever, and nobody's conceding that to them. Yet, Orac seems ready to concede the fight to define 'integrative medicine' to the quacks, as if it's already a done deal and they own the term. It's not, and they don't. The concession in the OP is the worst move possible.
Pretty much every institution doing anything could be doing a much better job assisting their clients. The obstacle is finding the necesary resources to do so.
How much would it cost society to underwrite training enough physicians to reduce the average patient load to the extent they could accomplish their primary function of providing physical support (delivering effective treatment for their illness or injury) and while being able to also provide the desired psychological support?
To what extent would we be willing to subsidize physician's revenues to the extent they could make an acceptable living while still being able to pay off the debts incurred in order to be trained as a physician?
I think every physician would love to have the luxury of spending as much time as needed with each and every patient, to deliver not only state of the art medical care and also provide the psychological support they need and desire. Given the reality of having to earn a living while covering the expenses of operating practice (salaries for nurses and aides, insurance, capital equipment, etc.) while retiring the debt associated with their education--well, I beleive someone once said "Ain't nobody got time for that!"
I think instead SBM should aggressively drive home the message that 'integrative medicine' is simply a synonym for woo.
My physician's office group has done something about treating the whole person in a way the doctors do not have time for: They have an RN care coordinator who deals with patients like myself who have chronic problems. I see her about every two weeks. My visits to her are free. She checks my vitals, we talk about my issues, and if there's a problem she feels needs the doctor's attention - med adjustments, pain, etc. - she either sets up an appointment for him to see me or she talks with him and gets back to me, or his nurse does. This works remarkably well. When I have an acute situation, of course, like my recent sinus infection, I see the doc and get my antibiotic or whatever is needed. This works remarkably well, probably saves the clinic, and the network of clinics to which they belong, a fortune, and results in a good quality of care, not to mention sparing the doctor from hand-holding time that could be better spent treating serious issues. I expect to see much more of this in the future. It's an excellent solution, as near as I can tell. For the first time in my life, I feel like I'm getting care instead of being out there on my own. And no woo involved whatsoever. Just good nutrition advice and other basics.
A chunk of the problem is the insurance companies, yes. Sometimes the physician recommends talk therapy, and the patient is willing, but the insurance won't cover it. If my doctor says I would benefit from massage, that comes out of my own pocket. So does a dietician's help in coming up with an appropriate diet that the patient will actually eat.
Telling people they should exercise is included in the general office visit, yes. They can probably even tell me why. But details on what might work take time that the doctor might not have, and that's not most doctors' area of expertise. Details don't just mean "try lifting weights" or "a lot of my patients like yoga," but teaching them what to do. A different skill set, and time-consuming. And you're not going to get that from a homeopath either, but somehow nobody blames them for that.
Are these bi-weekly visits free to you (i.e., there's no co-pay)but re-imbursed by your insurance carrier? Otherwise, i don't see how employing an RN full-time who isn't generating revenue could result in saving the clinic any money.
JGC @22 -- I heard an NPR report a while back about outfits that take care of older folks using a "capitation" model (I think it was) in which they're paid a fixed fee for every patient with some big incentive to keep them healthy. They used various ways of heading off acute problems, e.g. home health aides to check on people to keep problems from becoming acute and requiring expensive hospitalization. Unfortunately fee-for-service doesn't incentivize this -- you can make tons of money by treating your patient as a walking ATM, and some physicians unfortunately do just that.
JGC #22 - Yes, they're free. The feeling at the clinic is that they help keep the patients healthy and don't eat up the time the doc could be spending treating sicker patients. It's probably an attempt to compete with the spreading woo and problematic chiropractic.
The doc is spending time dealing with patients and not spending time talking to them about their diet and exercise and anxieties and every little poop crosswise. I'm sure the nurse is making considerably less money than the doctor, who can see more patients because he is taking less time blabbing. Patients who need things like steroid knee shots - which I had recently - and other well-paid activities.
Not that this isn't a good model, or that freeing physicians to treat those who most need/will most benefit from his expertise isn't a good thing of itself, but I don't see how this would likely result in any real cost savings for the clinic, unless the doctor can then squeeze in enough additional 'sicker' patients to offset the salary/benefits/insurance costs associated with employing a full time RN to deal with these patients.
palindrom @23 - ...you can make tons of money by treating your patient as a walking ATM, and some physicians unfortunately do just that.
Is this actually common? I've heard people complain that doctors don't give advice on nutrition (or not the "right" advice) or exercise or whatever because they want to keep their patients and keep making money off of them. This strikes me as silly, considering that medical school, residency, and all that is a pretty hard, time-consuming and expensive thing to do when you could just get an MBA and make a lot more money.
Also, there are 893,851 practicing MDs in the US, a country of 316 million. It doesn't really seem to me like they need to drum up business.
I'm basing my remark on an article from the New Yorker, maybe a year ago, by (very likely) Atul Gawande. The author (whoever he was) pointed out two Texas towns with similar demographics and wildly different per capita medical expenses as measured by (if I recall) medicare. The town with the high expenses had a fancy clinic with an attached imaging facility owned by -- you guessed it -- the clinic doctors. I suppose most of the imaging tests they ordered were justifiable at some level, but they sure didn't try to contain the costs. Au contraire!
JP@26 -- Nurse practioners make much less per hour than MDs, I'm afraid. Also, it depends on what the MD is doing with the extra time. Reimbursement is highest for MDs who perform procedures of various kinds -- consultations are reimbursed at a significantly lower level. If you can keep your MD's hands busy by shunting routine consults off to NPs, it's not at all unlikely that you'd come out ahead.
Ach, in #28 I meant to reply to JGC @25.
Incidentally, I am not a health care provider, but a very close associate of mine is.
I hear quite a bit about these issues, as the clinic administration gradually tightens the screws on their providers -- pressure to see more patients, generate more documentation, and obtain more reimbursement, while giving lip service to quality, without any corresponding commitment of resources.
Many of the undergrads I teach are pre-meds; I tell them to be certain to evaluate exactly what's involved before they commit. Medicine as it's administered these days strikes me as a pretty unattractive career choice for most people, unless they're the kind who were put on earth to be doctors.
Palindrom @23: Yes, "capitation" is correct. That type of payment model says you get $X to treat each patient, so it's probably in your best interest to apply every preventive thing you can think of. (And avoid taking on sick patients, which is where the model gets challenging). If I'm remembering my Health policy class correctly, this model (similar to the HMO) was actually illegal in the US for quite a while, because of fears of communism. (Group Health in Washington and Kaiser Permanente in California were the exceptions.)
In terms of money saved and quality of care it is clearly better, but it requires major changes in how all of the staff (MDs, RNs) get paid and it's hard to change a system that's been in place as long as fee-for-service.
sadmar,
I have ignored your previous digs at Dawkins, but this one intrigues me:
I would be interested to know where Dawkins has made anything even remotely resembling such argument.
^ "such an argument"
I'm not feeling up to my usual locquacity, so on the subject of trying to redefine "integrative medicine" to our purposes, I'll simply quote one of the best authors alive, Lois McMaster Bujold:
I'm still hoping that sadmar will show me where Richard Dawkins claimed that:
The closest I can find is the following, in an interview:
I don't necessarily agree with Dawkins' argument, which seems to me to be a variant of the slippery slope argument, but it doesn't appear to me to be arguing for people to "kill all the towelheads before they kill us". Yes I know this is rhetorical hyperbole, but it seems to me it's based on a fundamental misunderstanding of what Dawkins has written and said.
Kreb:
I was just trying to come up with an IRL example of the fallacy, and the anti-Islam take was the first thing that came to mind. I wasn't trying to dig at Dawkins. Dawkins has apparenttly 'walked back' his categorical condemnation of Islam. http://tinyurl.com/n3vvdzf
And AFAIK, he never articulated a full argument — spreading various comments among different Tweets, asides in this discussion or that, posting articles by Jerry Coyne on his blog, etc. I probably should just have said Sam Harris, as he does put it all together, or Coyne, but he's not famous enough to poke fun of.... And, again, RD himself has not, afaik, argued directly for a miliarist response, though Harris and Coyne have done so (at least in so many words...) He certainly hasn't raised any cautions about armed involvement in the Mideast...
RD did say, in the past, "I think Islam is one of the great evils of the world." And that argument is inherently based on the brutality exhibited by certain segments of the Muslim population... while ignoring the behavior of the majority of Muslims (who live in Asia, not the Mideast). But I'm really not interested in busting RD's chops.
[That said, the argument in the Telegraph article you quoted is pretty batty. It's simply false that religious moderates assert "‘that’s my faith, I believe it, you’re not allowed to question it and you’re not allowed to ask me why I hold it." See Terry Eagleton's critique of 'The God Delusion'. http://tinyurl.com/yca5e9n]
.......
The generalization from 'some of a category' to 'the category in general' is so common, I probably see it once a day, mounted by all sorts of folks for all sorts of positions. (I'd say we could name it "PGP's Fallacy", but that would be mean.)
I've probably thought of a dozen not-so-contentious examples I could have used instead since I hit the 'Submit Comment' button on #31, but I'm battling a nasty head cold at the moment, and I can't remember what any of them were. :-(
...........
And, fwiw, most of the "digs" I've dropped on RD were meant more as "Tonight Show" type jokes — i.e. Carson and Leno weren't partisan, they'd just take any opportunity to poke fun at the foibles of anyone with a high position in the public eye.
Are Doctors using all the good tools? An example: Thermography, the use of Infra Red to make visible areas on the body that are inflamed and could be sites for the beginnings of cancer. A lead time of years before mammogram identifies a cancer. The new 3D mammography system is being installed at a local hospital at a cost of about $130,000. A Thermography system could cost maybe $20,000 including camera and room requirements. "No it is not an approved system" by Health insurance providers and Doctors, I am told. Yet Who is working to provide approval and facts? Not the instrument provider! Not the Doctor, Not the Hospital, nor the drug companies. How can such a system be identified and installed?