
A recurring theme of this blog is to shine a light on what I like to call “quackademic medicine.” I didn’t invent the term, but I’ve made it mine. Basically, quackademic medicine is a term that very aptly describes what’s going on in far too many academic medical centers these days, which is the infiltration of pseudoscientific medicine and outright quackery in the form of “complementary and alternative medicine” (CAM). Of course, the more recent term for CAM is now “integrative medicine,” which was coined to imply the “integration” of alternative medicine with science-based medicine as though they are equals. Thus, there are academic medical centers that embrace acupuncture, reiki, and naturopathy, the last of which includes homeopathy as an integral part of its curriculum and skill set.
Among the centers of quackademia, of which there are far too many in existence, George Washington University is among the most egregious when it comes to embracing pure quackery. The last time I discussed GWU, I noted that the Center for Integrative Medicine at the George Washington University Medical Center (GWCIM) offers services that, charitably, be called pure quackery: acupuncture (of course!), chiropractic, craniosacral therapy, infrared light therapies, glutathione infusions, Myers’ Cocktail, naturopathy (again, of course!), reiki, intravenous high dose vitamin C, and genetic profile results that include “customized interpretation of 23andme.com genetic profile results with specific accent on methylation and detoxification profiles.” Some of these are quackery. Some are “rebranding” lifestyle interventions as somehow “alternative” (and therefore much more hip). Some blur the lines between the two, such as “functional medicine,” a branch of CAM that combines “wholistic” medicine with a whole lot of lab tests and supplements to correct abnormal lab values. The Cleveland Clinic is especially enamored of functional medicine.
Now I learn that GWCIM has recently added another questionable treatment to its already expansive list of questionable protocols. No, the protocol to which I’m referring is not homeopathy, craniosacral therapy, or high dose intravenous vitamin C. The kindest way to describe it is experimental, even though it seems to be offered to anyone without a clinical trial. As it is experimental, it is unproven. It’s also based on pretty thin gruel as far as clinical data goes and resembles to me the premature use of 23andme genetic profiles to guide care before we even know what these profiles mean. No, strike that. It reminds me of functional medicine:
Muses Labs announced today that it has partnered with the George Washington Center for Integrative Medicine (GWCIM) to offer the MEND™ Protocol to patients located in Washington, DC. This agreement allows individuals with pre- and early-symptomatic cognitive decline, as well as mild Alzheimer’s disease patients, to benefit from the MEND Protocol via the Center’s Mental Health program operated in collaboration with the George Washington University Memory Clinic.
The MEND Protocol is a data driven, technology enabled, personalized methodology to correctly identify and simultaneously treat the dozens of pathology drivers of age-related cognitive decline. The MEND Protocol is designed to help patients who are beginning to have symptoms of age-related cognitive decline, those with a family history of dementia and patients with mild Alzheimer’s disease. The Protocol recommends optimal medical interventions personalized for each patient and has the potential to improve memory and cognitive function. The MEND Protocol is an emerging methodology that reflects a new approach to addressing complex diseases.
The MEND™ Protocol is a treatment for Alzheimer’s disease marketed by Muses Labs. I always become very suspicious when I see marketing materials that make claims like this:
MEND™ Protocol simultaneously applies multiple medications and lifestyle changes in a highly-personalized manner to attempt to halt and reverse mild cognitive impairment (MCI) and early stage Alzheimer’s disease. MEND Protocol utilizes existing FDA-approved drugs, supplements, lifestyle changes, and medical markers and tests in a novel manner. Personalization of the protocol depends upon an individual’s genome, medical test results, comorbidities, current medications, medical history, and other inputs.
MEND Protocol is designed to address the active underlying pathways for Alzheimer’s disease including metabolic issues, toxicity, inflammation, and mitochondrial damage. Due to the complexity of the personalization process, the Protocol is realized via health management software. The algorithms are able to incorporate logic to process a wide range of data on an individual’s health status and recommend specific interventions matched to the etiology of an individual. The recommendations are different for each individual and change over time.
Ah, yes, “personalized” medicine and a “personalized” protocol. Muses Labs claim to use these factors to design a personalized treatment for MCI due to early stage Alzheimers:
Based on the recognized causes of cognitive decline, the MEND Protocol collects individual patient biometric and behavioral data, including:
- Genome
- Bio-specimen data
- Medical history
- Demographics
- Medications
- Patient lifestyle
- Cognitive ability
The MEND Personalized Treatment Plan is provided to both the physician and the patient, so they can review the results together. The physician prescribes the treatment plan as appropriate. Patients are periodically retested and the treatment plan is updated over time.
You know, this protocol smells of questionable science. My skeptical antennae start really twitching when I read things like “toxicity,” “inflammation,” and “mitochondrial damage.” It sounds very much to me like “autism biomed” coupled with an appeal to genomics and computer algorithms. They start twitching especially hard when I see images like these on a website:

Yes, its’ a scientist in a white lab coat apparently manipulating a DNA double helix with his hand, complete with a white light that makes it look as though he’s shooting energy from his fingers. OK, it’s not quite that blatant, but it’s close. Star Trek fans might remember a term frequently used to describe some of the scientific discussions that occurred on the show, namely “technobabble.” Basically, technobabble consists of impressive and scientific-sounding jargon that, when examined more carefully, turns out to be basically meaningless.
This next part of the description of the MEND protocol might not be technobabble, but it is pure woo babble. Its very name (metabolic enhancement for neurodegeneration, abbreviated MEND) tells me that. So does this next bit:
The analysis algorithm recommends both pharmacological and non-pharmacological components. For example, if synaptic reconstruction and maintenance is needed, then multiple biological mechanisms may require normalization, enhancement, or administration. Examples of these underlying biological mechanisms include: periodically activating autophagy, blocking prionic tau amplification, increasing beta-amyloid clearance, inhibiting beta-amyloid oligomerization, minimizing inflammation, normalizing neurotrophic factors, reducing ApoE Ɛ4- mediated signals, reducing stress, reducing tau phosphorylation, restoring cholinergic neuro- transmission, and reversing memory loss. Assessing the status of these biological mechanisms involves quantifying and observing hormonal balance, citicoline, C-reactive protein and other inflammation-related markers, diet, exercise, homocysteine, omega-3 acids, sleep, and so on. Interventions targeting specific biological mechanisms are then prioritized and prescribed to optimize key biological mechanisms. Medication doses are specified to an individual’s needs. Individuals are re-tested periodically and the protocol is updated as necessary.
What the hell does this even mean?
Whenever I see claims like this, my first instinct is to go to PubMed. At the very least, I expect to find a list of publications on the company website. So, before going to PubMed, I perused the Muses Labs website. All I could find was one publication. Before I get to that publication, though, let me just take a look at some things I found using the almighty Google search. I can’t help but note that all the articles I found using Google mentioned the very same single publication.
As you probably know, Alzheimer’s disease is a form of dementia, of cognitive decline, related to aging. It isn’t (yet) known what causes it. It’s known that Alzheimer’s disease is a chronic neurodegenerative disease. It’s progressive and relentless and the cause of up to 70% of cases of age-related dementia. The cause of the disease is not well understood at all. It is known that Alzheimer’s patients tend to have amyloid plaques (amyloid is a protein) and neurofibrillary tangles in the brain. Currently there are no treatments that stop or reverse its progression, although some can temporarily reverse its symptoms. It’s a horrible, horrible disease, one that I can’t help but fear as I get older. When I have a lapse in memory, I have a tendency to joke about “early onset Alzheimer’s,” but it’s no joke at all. Alzheimer’s dementia is just about the worst fate I can imagine.
Muses Labs itself touts its approach thusly:
The approach we’re employing relies upon advanced software and big-data analytics, and incorporates decades of medical research. Muses Labs offers a service that utilizes the Internet and information technology innovations to make the Protocol practical and accessible to individuals with cognitive decline around the world.
Elsewhere, the company is described thusly:
The company says this approach to Alzheimer’s disease (AD) is based on the molecular biology of the brain and the bodily systems that support it. Decades of scientific research from around the globe are brought together and incorporated into MEND. Muses Labs combines medical expertise with software algorithms. Its algorithms figure out the optimal personalized therapy for an individual, and enables their physician to prescribe the therapy. Muses Labs software then motivates an individual’s adherence to the therapy it recommends.
All of this sounds all very nice and impressive, and there are indeed legitimate scientists on the Muses Labs editorial board, although there is also Dr. Mikhail Kogan, who just so happens to be the Medical Director and the Integrative Medicine Fellowship Director at the George Washington Center for Integrative Medicine, Washington DC. Not surprisingly, he also does geriatrics and embraces functional medicine. Come to think of it, this whole Muses Lab approach reeks of functional medicine, which I like to characterize as “making it up as you go along,” because of its reliance on lots of lab tests whose interpretation is questionable. In this case, we appear to be seeing functional medicine expanding into genomics.
Still, as many red flags as I see in the press releases and Muses Labs literature, it is always possible that the company is on to something. It’s not incorrect when it says that Alzheimer’s disease is very complicated, nor is it incorrect in its assessments of the current “state of the art” that single agent therepeutics have largely failed to reverse cognitive decline. However, it does not follow from that that the MEND protocol works. We’ve been using systems biology approaches to try to develop better treatments for various diseases for at least a decade now, and, in cancer at least, the results have been mixed. There was a lot of hype and hope at first, but it wasn’t long before that hype and hope ran straight into the wall of the implacable biology of the disease. So what’s the evidence for the MENDS protocol?
So let’s take a look at the publication that Muses Labs touts as evidence that its protocol is so promising as a treatment for early Alzheimer’s disease? Given that it’s the only study. It’s also a single-author paper, which is pretty unusual for any sort of case series or clinical trial. I know nothing about the author, Dale E. Bredesen, other than that he is affiliated with the Buck Institute for Research on Aging and UCLA’s Mary S. Easton Center for Alzheimer's Disease Research. It’s obviously a pilot study; in fact, it’s a small case series of ten patients treated with the MEND protocol.
This case series was immensely unsatisfying to read. It’s open access; so you can read it for yourself if you don’t believe me. I wanted to know more. I wanted to know just what the heck the MENDS protocol entailed. Unlike most papers reporting the results of case series or clinical trials that I read, this paper was very thin on the details. For example, this table describes it (click to embiggen):
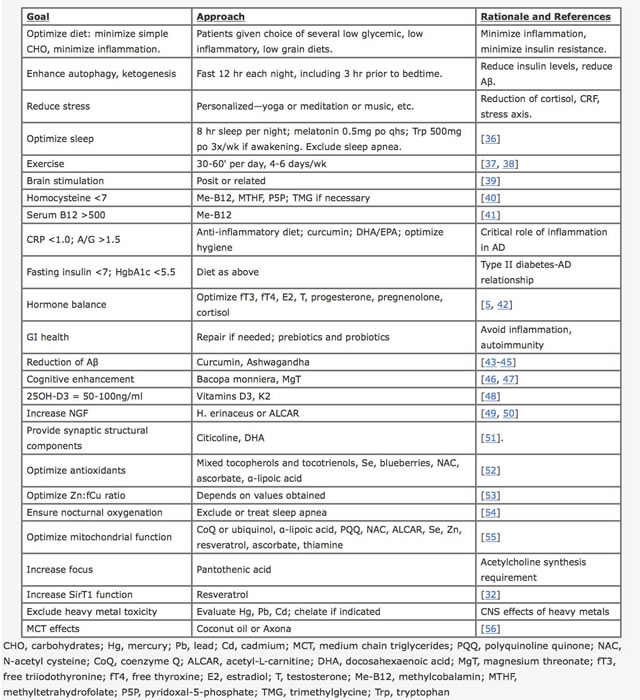 The MEND™ protocol: Sure looks impressive and science-y, but it it either?
The MEND™ protocol: Sure looks impressive and science-y, but it it either?
Patient #1 is a 67 year old woman with two years of progressive memory loss whose mother had developed progressive memory loss at roughly the same age, become demented, and ended up in a nursing home, not dying until she was in her early 80s. This was the regimen she was placed on:
As noted above, and following an extended discussion of the components of the therapeutic program, the patient began on some but not all of the system: (1) she eliminated all simple carbohydrates, leading to a weight loss of 20 pounds; (2) she eliminated gluten and processed food from her diet, and increased vegetables, fruits, and non-farmed fish; (3) in order to reduce stress, she began yoga, and ultimately became a yoga instructor; (4) as a second measure to reduce the stress of her job, she began to meditate for 20 minutes twice per day; [5] she took melatonin 0.5mg po qhs; (6) she increased her sleep from 4-5 hours per night to 7-8 hours per night; (7) she took methylcobalamin 1mg each day; (8) she took vitamin D3 2000IU each day; (9) she took fish oil 2000mg each day; (10) she took CoQ10 200mg each day; (11) she optimized her oral hygiene using an electric flosser and electric toothbrush; (12) following discussion with her primary care provider, she reinstated HRT (hormone replacement therapy) that had been discontinued following the WHI report in 2002; (13) she fasted for a minimum of 12 hours between dinner and breakfast, and for a minimum of three hours between dinner and bedtime; (14) she exercised for a minimum of 30 minutes, 4-6 days per week.
How we get from “systems biology” to yoga, exercise, weight loss, enough sleep, and a better diet is unclear. You don’t really need systems biology to suggest that these interventions will at least improve health and might slow cognitive decline. As for going “gluten-free”? On what rationale was that intervention based? I have the same questions regarding fasting and the vitamins. Basically, reading the relatively vague description of the MEND protocol provided here, I see nothing that requires all that fancy systems biology and those computer algorithms touted by Muses Labs. How “data-drive” and “big data” do you have to be to come up with this protocol?
Another failing of this writeup should be obvious to anyone who routinely reads (and especially to anyone who participates in) clinical trials. What were the objective outcomes? Even in a case series, there are usually some objective outcomes examined. For example, did they do various tests of cognitive function before and after, in order to determine if there was any objective improvement. How was the diagnosis of cognitive decline nailed down. Of the three (out of ten) patients described, patient #2 is the only one whose workup for Alzheimer’s disease was described in anything resembling in depth, and there is no report of any followup tests, just the patient and wife’s reports of his improvement. Basically, nine of ten patients reportedly demonstrated “objective or subjective” improvement, and six were able to go back to work. That’s nice, but where are the results of the full dementia evaluations, complete with standardized cognitive assessment examinations before and after the MEND protocol intervention? This case series really needs some meat on its bones before it will persuade me that there might be anything to this protocol. As it is, it sounds like one of any number of studies and case series published in CAM journals: Long on description, short on concrete reporting and controls.
As a pilot study, this sounds on its surface mildly promising, although it is really hard to tell given the lack of description of anything resembling something a clinical scientist would want to know to judge if further study is needed. Maybe it is. Maybe it isn’t. Another disturbing thing about this paper is that there is no mention of institutional review board approval, making me wonder if this was IRB-approved. Even a retrospective case series needs IRB approval, at least before publication, and this doesn’t seem to have it. Searches of Clincaltrials.gov failed to find registered clinical trials of the MEND protocol.
Maybe this protocol is worthy of further study. Maybe it’s not. I can’t tell for sure if it is based just on this paper and Muses Labs hype, both of which have enough red flags in them to make me think that the MEND protocol is nothing more than functional medicine on steroids. Whatever the case, however, I can be convinced, but not by this thin gruel. If Muses Labs and, presumably, GWCIM, are ever going to find out whether its protocol works to halt or reverse early cognitive decline in age-related dementia caused by Alzheimer’s disease, they should stop putting the cart before the horse and treating patients with an unproven protocol outside of the context of an IRB-approved clinical trial protocol. They should do the hard work it takes, get a protocol IRB-approved, and do the clinical trial before offering the MEND protocol to just anyone off the street suffering from early Alzheimer’s. That’s how you find out if a new protocol works. The MEND protocol might not be quackademic medicine, but how it’s being sold sure feels like it.
Oh, and try not to fetishize computer algorithms and systems biology so much. Nothing in the MEND protocol that I can see depends on either.
"This agreement allows individuals with pre- and early-symptomatic cognitive decline..."
Someone educate me. What is "pre-symptomatic cognitive decline?" Is that not something that, by definition, is not diagnosable?
Has the IRB weighed in on this? It sounds highly ... irregular.
One, I don't think "data driven" means what they think it means.
Two, a "personalized methodology" involves lots of N=1 cases. How do they get any kind of statistical power to determine whether the methodology works better than a control or placebo? I'll grant that it makes it impossible to disprove their hypothesis, but in medicine the burden of proof is (or should be) on the researcher(s) investigating a prospective new treatment.
Good catch. I didn't notice that. :-)
Looks like I picked the wrong week to quit wishing violence on quacks.
Pre-symptomatic cognitive decline could be detected by neuropsych testing, I guess. As long as the person does not complain of memory problems, they have no symptoms, by definition. Perhaps what they meant to say is "mild cognitive impairment," which is worse than normal age memory loss, but not full blown dementia. It is all part of a spectrum.
Well, the case study mentioned, the patient begins this protocol at age 67 and doesn't follow all the dictates in the program. So if the patient doesn't comply with the full program, how can we evaluate it?
But what I don't see is, how did the patient's course compare to the course of similar patients with Alzheimers? Yeah, she reported some cognative improvements over a couple of months but how do we know that's not the placebo effect? Alzheimers develops over a long period of time; where will she be in three more years and where is she now?
And were they on Aricept or Namenda during this trial?
God forbid this patient should eat a farmed fish.
Oh man that guy!! Saw Bredesen give a talk at a conference one time and the level of bizarre/crazy was strong with that one. He really came across more as a snake oil salesman than a scientist with his mysterious 20-step protocol or whatever it was.
Orac, this post is - in my humble opinion - wanting in its level of insolence. Or should I say that this MEND protocol seems to me to be deserving of a heapin' helpin' of it.
The whole thing seems to be a word salad. How does one determine if synaptic reconstruction and maintenance is needed? How does one then reconstruct a synapse? And how might biological mechanisms be administered? How does yoga block prionic tau amplification - or is it the veggies that do that? Maybe yoga is more involved in inhibiting beta-amyloid oligomerization? And this is being made available to real patients on the basis of 10 case studies which don't even include objective tests of cognitive function.
What a crock.
It's late, I'm tired and maybe I have my cranky pants on, but "the MEND protocol might not be quackademic medicine, but how it's being sold sure feels like it" seems too polite.
I'm not a neurologist or expert on Alzheimer's, and, unlike the case with vaccines, I haven't studied the issue to be as confident discussing it as I am discussing vaccines. So I toned it down a bit, in case I was in error about anything. Remember, a man's got to know his limitations:
I also didn't know that Bredesen was so full of woo, but I should have suspected it and spent some time Googling his name and reading some of his stuff. Another thing I had wanted to look into was the journal, but it had an impact factor of over 6, which makes it seem unlikely to be a truly woo journal.
Unfortunately, I am all too aware of Alzheimer's woo courtesy of PRN.fm.
Actually, the head honcho's woo is remarkably similar with a few differences:
more exercise ( an hour a day), no fish ( truly vegan), no HRT ( the demon's brew), loads of supplements, some targeting the brain ( like NAC) and powdered fruit and vegetables ( all conveniently sold at the website's store).
About the 'pre-symptomatic decline':
this woo holds that aging begins at age 27- it's early old age or suchlike. He gets people to label normal everyday forgetting ( I studied this stuff- believe it or not) as precursors to dementia. He usually tells and re-tells a story about a wealthy friend who didn't follow his advice and who keeps asking the same questions over and over; in addition, he has a testimony from a supposed professor of art history who has 'advanced AD' and whom he 'cured'.
And preventive woo is also out there. Same products, same protocol.
Unfortunately as well, my friend just had to fly to Ireland because her sister, not at all aged, developed AD - seemingly mild- but died of pneumonia within 6 months.
In other news...
Dan Olmsted has responded to me ( at the most appropriately named, " A particularly odious antivaccine 'warrior'... post ). He doesn't like experts it seems.
OT but it's Friday and getting later all the time, there are more than 10 comments and I have to leave soon because of an appointment...( is that enough?) so I ask whether braggadocio from an accomplished woo-meister is EVER truly OT at RI?
I would guess NOT.
Orac's non-fanboi, Mikey, is announcing that his new book is #1 at Amazon/ Science and Math. There will be a follow-up about pesticides. I can hardly wait.
The paper from Muses Labs notes:
He received Federal funding (not to mention the affiliation with UCLA), which therefore means the study is covered by the Common Rule and requires IRB review and approval. No mention is made in the paper of any ethical review.
What's worse, cognitively impaired individuals are considered vulnerable populations. 45 CFR 46 requires researchers and IRBs to include additional protections for the subjects.
"reducing ApoE Ɛ4- mediated signals"
How on Earth do you do that without installing profound dyslipidemia? It is theoretically possible (ApoE Ɛ4 polymorphism is associated with AD without dyslipidemia, so it's not like an ApoE loss of function), but I've never seen anything like it. Heck, I've never seen a researcher actually knowing what was in that polymorphism that did not prevent metabolic function but created the early-AD phenotype.
Bredesen has a new paper out. There's a link for it in this article. He's saying that he now has brain scans to 'prove' his protocol works. I haven't looked at the paper yet. I'm not sure I will - because it doesn't matter. His experiments have no controls as far as I can tell. It's incredibly bad science.
It's time for institutions like UCLA, the Cleveland Clinic, Johns Hopkins, George Washington - and too many others to name - to stop enabling this bad science. I find it difficult to believe that without a UCLA credential, Bredesen would have been able to publish this mess in anything other than a pay-to-play journal. But I'm a chemist and not all that familiar with the way medical publishing works - I could very well be wrong.
To me, this protocol is no different than what naturopaths do - throw supplements and diets at a problem willy nilly and take credit when the patient gets 'better.' And use terms like 'holistic' and 'combination therapy' and 'systematic' to try and make it sound more palatable and scientific.
Here's the link: https://www.sciencedaily.com/releases/2016/06/160616071933.htm
Heh. My timing's bad. The press release is yesterday, and I might have seen it. But unfortunately I didn't.
This putative trial has gotten a lot of publicity, entirely out of proportion to its merits.
Here's the Buck Institute press release:
http://www.buckinstitute.org/buck-news/Memory-loss-associated-with-Alzh…
Here's the UCLA press release:
http://newsroom.ucla.edu/releases/memory-loss-associated-with-alzheimer…
I would not call this a trial. Of the 10 subjects, each got a different set of putative therapies. The therapies sound like something you'd get at Whole Foods: gluten-free diet, probiotics, grass-fed beef, organic chicken, fish oil, CoQ10, yoga, music, meditation, fasting, etc. At best, I'd call this a study, and not one that should be taken very seriously. It's based on a dubious notion -- that monotherapies have failed, so we should try a whole bunch of therapies at once. There's no control group, the researcher seems to have evaluated the subjects' responses to treatment qualitatively in 7 cases, and the conclusions go far beyond any reasonable interpretation of these meager results.
Isn't this software considered a medical device? Medical devices are regulated by the FDA, so if this is a medical device there should be a filing for it.
The idea isn't completely out of left field. There is a general consensus that most mathematicians do their best work before the age of 30. Einstein, for example, was 26 when he published the paper for which he was later awarded the Nobel Prize, but went down a number of blind alleys (e.g., unified field theories and "God does not play dice") starting in the mid-1930s. It's also well known that adults find it much harder than children to learn another language, though this is more of a a steady decline in that ability (e.g., one of the reasons Navajo code talkers were used in World War II is that the language is nearly impossible for somebody starting after the age of two to learn).
Of course, as is usual with woo that has a small element of truth to it, it is likely that this guy takes it much too far.
"The MEND Protocol is a data driven, technology enabled, personalized methodology to correctly identify and simultaneously treat the dozens of pathology drivers of age-related cognitive decline."
So much technobabble right out of the gate. Brutal.
@Debra M.
Looks like another bit of research for which Bredesen and his team did not report IRB approval.
I haven't yet read the whole paper in depth, but did look over patient 1. It's reported that:
Bredesen explains that the episode of memory loss is because Pt 1 stopped the protocol. It is equally possible that Pt 1 stopped the protocol due to AD. IIRC, AD has alternating episodes of memory loss and lucidity, with poor cognitive function becoming an increasingly frequent event.
With no controls, and no methods described, the paper is useless with regard to drawing any conclusions on efficacy.
Todd W@22:
a.k.a. Always plame the patient, never the treatment. Where have we heard that before?
Let me first say I love this blog.
I think this, however, is a case of you throwing the baby out with bathwater. I don't see any connection of Dale Bredesen, or any of his co-authors, to Muses Labs at all…
Dr. Bredesen is very reputable researcher, who beyond doing these case studies finds time to publish many other pretty interesting papers, like this one about APOE: "http://www.jneurosci.org/content/36/3/685.short".
Also, Mark Thorson, in the comments you claim that "it's based on a dubious notion — that monotherapies have failed, so we should try a whole bunch of therapies at once." Where is your evidence that this is a dubious notion?
I actually believe combination therapies are incredibly underexplored… There are obvious reasons why they are underfunded in industry, such as IP issues, and an inability to quickly obtain data necessary for approvals. They can also be challenging to execute, especially with protocols as ambitious as this one. But even very senior execs in industry believe they could hold a lot of promise.
I haven’t had time to read the latest paper in detail either, but it definitely appears to beef up the objective and quantifiable measures. I realize it is not a RCT, but this is clearly the direction the authors would like to go, as they write “The results also support the need for a large-scale personalized clinical trial using this protocol.” It is still preliminary data, but promising, and especially given it’s in such a serious disease like Alz, and one that is littered with so many high-profile failures of monotherapies. Let’s not let perfect be the enemy of the good!
Irrelevant. Linus Pauling, Brian Josephson, and Sallie Baliunas[1] (to name three examples off the top of my head) were once well-respected researchers, too. That was before they involved themselves in various pseudoscientific pursuits: Vitamin C as cure-all, extreme racism, and climate science denialism, respectively.
I have no idea whether Bredesen published good science in his younger days--I'm not qualified to evaluate it myself. But he's clearly gotten into some disreputable stuff lately. If he really had anything promising, he would be working toward setting up a full clinical trial with enough patients enrolled to have some statistical power for determining whether the protocol(s) is(are) more effective than placebos. And he would make sure that he had IRB approval for this clinical trial. He wouldn't be mucking about with case studies that don't have IRB approval. He should know better, else he would not have obtained or kept a position at a reputable school like UCLA.
[1] I recall that Baliunas gave a colloquium in my Ph.D. department when I was a young grad student. Her research focus was on solar physics. This was before she started collaborating with Willie Soon to produce a series of easily refuted papers on the Sun's influence on the Earth's climate.
Bobby Brooke #24
I won't comment on the rest of your comment as I want to read the paper first, but I am wondering if you actually looked to see if there was a connection between Dale Bredesen and Muses Labs, because it took me less than a minute to find this page, which clearly indicates his extremely strong connection to Muses Labs:
https://webcache.googleusercontent.com/search?q=cache:deRFQ6OfDYAJ:http…
It seems he stepped down in 2015, but that was after this paper was released
http://www.prnewswire.com/news-releases/dr-dale-bredesen-announces-term…
@Travis
One notes that in the original study solo-authored by Bredesen, which Orac linked to, he declares he has no competing interests. However, the MEND Protocol was developed by him and Muses Labs, so he conceivably stood to make money if the research supported his claims. A quick scan of the paper found no mention of Muses Labs or Dr. Bredesen's connection to it.
@Todd W,
After writing my comment I thought to check, which I should have done earlier, and noticed the same.
Looking at the journal's CoI statement, it seems like his connection to Muses Labs should have been made clear.
http://www.impactaging.com/forAuthors.html
Wouldn't getting the recommended amount of sleep generally help your cognition? (Patient #1 went from 4-5 hours of sleep to 7-8.)
And I know my dentist is in love with electric toothbrushes (and water picks), but even he wouldn't try to claim it will prevent dementia. How would that even work?
@Travis #26
I did look, but only at their website, so many thanks for showing that he may have been involved at one point, but that he terminated his relationship with them. Beyond that, the press release writes that he "severed all professional and scientific relations with Muses, including all professional and scientific relations with Muses, including consulting, trial participant review, and any interpretation of Muses information." This does not look amicable in any way, so he has clearly distanced himself from this group.
The press release goes on to describe him setting up his own company, MPI Cognition.
@Todd #27
I don’t believe what you write that “the MEND Protocol was developed by him and Muses Labs.” As you mention also, Dr. Bredesen is listed as the sole author on the 2014 paper. He doesn’t list conflicts of interest, but he does list in the acknowledgements his financial support from groups like UCLA, Buck Institute, Alzheimer’s Association, and private individuals. If I had to guess, I’d say he probably debated whether to list companies like that one, and MPI Cognition on this recent paper, but determined they didn’t meet the threshold. They most likely didn’t provide any financial support related to the research, and they’re so probably so early-stage that they haven’t provided him any consulting fees whatsoever. So even though he may have a title, it could still be somewhat debatable as to whether or not he really needs to list them. In any case, especially with this MPI Cognition company, it looks less like he’s trying to profit from it, and more like he’s trying to setup the infrastructure to recruit patients, run all of these assays necessary, and coordinate logistics to enable a large RCT to get more definitive proof that this regimen works.
@Eric #25
The paper on a surprising new molecular mechanism of ApoE4 (the single leading genetic risk factor for Alz) was published in January 2016, so hardly from “his younger days”. More on it is here: https://www.sciencedaily.com/releases/2016/01/160128155753.htm
@Orac #10 & #17
I hope you’ll read the latest paper and continue to revise and add relevant details…
@JustaTech #30
Yes, good oral hygiene for Alz sounds goofy to me, too, but lo and behold, there’s fairly decent evidence to support it: “http://www.medicalnewstoday.com/articles/264164.php”. It’s also an example of something that’s entirely without risk and could reasonably help, so why wouldn’t you do it? Where this gets more even more interesting is when regimens/protocols like this become the new norm, and all patients adhere to them, and then you can combine them with leading AD investigational treatments (i.e. even some of those compounds that failed when developed as monotherapies in the past).
Orac #10 - point taken. My cranky pants were definitely on (they're so comfy) - I had spent a good part of last evening reading _all_ the comments over at the SBM post on... I don't want to derail this thread by mentioning it... rhymes with 'fun patrol'.
And it seems you're damned if you do and damned if you don't - I complaint that you're too reserved, someone else complains that you're throwing the baby out with the bath water.
As a Learned Sage told me this afternoon on a different forum:
"All that data sounds really good if you did not develop (condition X) but if you were one of the one in two hundred twenty seven who did develop (condition X) then you would be really happy about subjecting everyone in your age group to (invasive exploratory procedure A) despite the weight of expert opinion against such screening."
The word 'smug' was thrown around a bit, not by me, and I am pretty sure that I did not manage to influence a single opinion.
@ Denice
Gah, it's now number 3, so I guess that was right at some point. And at some point, it was a number 2, but everything HWSNBN does is a number 2.
OTOH, Randall Monroe's excellent "What if" is number 8. That's something.
OK, I should stop posting off-topic now.
@ Eric Lund
Right. There's some stuff in cognitive about prime time for mathematicians, physicists et al and memory / learning.
BUT
I think that the hoary old woo-meister
is talking more about the hotness factor or suchlike for women. ( who according to his calculations are quite over and done early UNLESS THEY follow his protocols to the letter of the law)
@ Helianthus:
When I last looked his barrel of tripe ... I mean *book* was at one with Mukherjee trailing.
I'm a spy in the house of woo**
For the past two and a half months I've been suffering with a relatively minor but irksome injury- originally, I hurt myself whilst reading a menu in Portuguese when my sandal caught upon a broken paving stone during the financial crisis a few days after a flu vaccine.
I have since re-injured it a few times
HOWEVER this time it's taking longer and I began to lose patience. using anti-inflammatories, ice and mild exercise have all helped but I am not myself yet.
One of my gentlemen suggested various woo-fraught activities including acupuncture - I recoiled and mentioned toothpicks immediately-
HOWEVER there were hidden incentives in this altie programming schtick- it was Chinese therapy- not just acupuncture and SOMEONE else was paying***
So armed with cash and a cavalier attitude, I embarked on a suburban journey to the offices of a Dr Hsu ( not her real name) who has been doing this for 35 years in both a city and suburban locale- posh and semi-posh, respectively.
I filled out a long laundry list of possible complaints ( I actually have very few) and met the practitioner who was abrupt but cautiously friendly. I was told my tongue betrayed my 'low energy' and that I might need supplements ( which weren't mentioned later at all surprisingly). She started to press upon various points around my jaw and ears as well as down my leg where the problem was: her bony fingers poked sensitive spots - I suppose places where the Qi is blocked or suchlike. She carefully applied the disposable needles, unwrapping each one.
A few of the spots seemed quite sensitive but one near my knee felt really differently as she pressed and poked at it doggedly for a while. Then she applied a heat lamp aimed at the OTHER leg and left me to listen to Chinese classical music for 30 minutes.
My next 2 visits included more probing, needles and last but not least- CUPPING!- which was the be-all and end-all of woo. She placed more than a dozen mini glass fish bowl-like cups down my side and leg - some of which were rather discomforting and left marks ( fortunately, not the ones on my thigh which can be easily seen). I suppose it extracted the stagnant Qi or Evil as each one popped when she removed it.
All in all, I do feel better but first of all 2 weeks have past, I continued taking meds, doing exercises and drinking wine. I must admit that she did something when she pressed and fixated upon that one particular point near my knee on the first visit. My best guess is that she did something like the tui na practtioners- i.e. massage therapy / physiotherapy-like- and that all the rest was merely window-dressing. BUT I do think that she believes in it all.
** oh why not?
*** I never pay for woo in any way, shape or form
I'd really like to see the insides of these "algorithms". Something tells me they're basically just choosing a bunch of treatments in their database based on RNG and displaying them on screen.
Garou, several "deep learning" systems have appeared recently (Google's TensorFlow, Berkeley's Caffe, IBM's SystemML, and a host of others). Nearly all of these systems are freely available. I predict all sorts of meaningless misapplications of these systems , far more than from people who understand their use and limitations.
@ # 24 "Dr. Bredesen is very reputable researcher..."
Apart from the fantasy press releases, which in UCLA's case the central administration should look at in a misconduct inquiry, I would think that Dr Bredesen, or others close to, will have a small-cap start-up company somewhere not far from an IPO, selling personalised treatment programmes.
Conspicuously bullshit packaging of diet and exercise lifestyle improvements, may of which anybody who hopes to be in their right mind at 80 should adopt.
I think this is quite interesting from a medical/scientific perspective, but less so and more challenging from a business perspective. It obviously is not the traditional patented monotherapy pill-in-a-bottle approach.
In a perfect world / more efficient market, more rigorous programs like this might be really well rewarded, but there's so much overhyped research and supplements out there (plenty of good stuff, too, though) competing for people's attention, I would think it'd be tough.
In any case, maybe I'm naive, but the latest data (June 2016) look pretty interesting: "http://www.impactaging.com/papers/v8/n6/full/100981.html".
I saw that after I wrote my post (awesome timing, no, to have written a post the very same day that a press release touting a followup study came out?), and I do plan on writing a followup, perhaps for Tuesday or Wednesday. (Monday's post is already written.) It's not nearly as interesting as you think.
The more I read this stuff the more I am convinced that it concerns BUSINESS plans not research.
"You know, this protocol smells of questionable science. My skeptical antennae start really twitching when I read things like “toxicity,” “inflammation,” and “mitochondrial damage.”
Orac, to be fair those are indeed mecanism that are believed to be implicated in Alzheimer's dementia, especially mitochondrial damage and inflammation. "Toxicity" is a bit vague but i could refer to "neurotoxicity" caused by amyloid-beta and tau oligomerization in brain. What is mostly quacky here is the next part :
"Examples of these underlying biological mechanisms include: periodically activating autophagy, blocking prionic tau amplification, increasing beta-amyloid clearance, inhibiting beta-amyloid oligomerization, .... blablabla...."
-> Which is mostly a mixing of all the keywords associated with Alzheimer on pubmed.
To my mind the biggest red lights are a) the papers have not disclosed the exact treatment regimens, and b) MEND is a commercial "thing" before it's even been subjected to proper (RCT) testing.
Something else about that complicated treatment regimen:
The complexity of it could potentially be used as a set-up for "the failure of treatment was not the fault of the treatment regimen, it was the fault of the patient for failing to follow it exactly."
We have a phrase around here for that, that I can't remember at the moment (eeek!, early-onset AD;-) but also involves the element of "the patient didn't believe hard enough!" I suppose for patients whose brains are being eaten by AD, it's easy to "not believe hard enough."
My "alt med warning light" is blinking yellow.
-----
Denise @ 37:
I also had an opportunity to guinea-pig alt med on myself recently. A horrid cold with a vicious sore throat that would not go away. After a night of "sore throat was so bad I couldn't sleep," I thought "research opportunity to test some quacky stuff" since in my view of things, misery is more bearable when it's a chance to produce or collect information.
Long story short, I got some "Emergen-C" fizzy vitamin C drink powder (1,000 mg. vitamin C and 22 mg. zinc per dose), a particularly egregious-looking example of supplement woo. I gargled one packet during the day, one before bed. Woke up the next day with sore throat nearly gone. Gargled two more packets of the stuff that day, and the sore throat was completely gone the day after that. "WTF?!"
To my mind that was too pre/post for coincidence, and too clear-cut for placebo. The plural of anecdote is hypotheses; someone ought to run a controlled test to see if there's anything real to this. Then if it actually works, it should be adopted into evidence-based medicine quickly enough that alt-med can't get traction to claim credit for it.
It sounds to me like MEND is being healthy. Diet, exercise, that sort of thing. Adding FDA-approved drugs if symptoms. What's new in this?
I saw an article about MEND for the first time in the DailyKOS today. This really undermines my confidence in that newsletter.
Rather than knock down alternate methods, emperical evidence can be good enough when the results are achieved. The only problem with mono therapies are that they don't always work and there's a lot to be gained financially to convince a large population of people that it's all backed by science. There's emperical evidence that too many people get side effects worse than the treatment (and never cured) by allopathic methods, regardless of science. When you start nit picking for scientific studies things become muddled without seeing the results best given by the patients themselves. It's not all quackery. It's only quackery to those who don't bother to explore that maybe what they believe to be the best science isn't always the best for human outcomes. Furthermore, I say just follow the money trail, which isn't always a bad thing unless someone stands to lose something valueable from another's gain. Not having scientific evidence vs patient results is not one of them.
I very read plenty of publiahed studies on diabetics and found them mostly lacking in their initial setups, basically nullify ingredients the whole thing. I decided to use foods, diet changes and watching results long term
.....and found it more effective than pill therapies. This used on family members disgruntled with the confusion and side effects of scientific studies.
Goldie: where does the money trail for all those supplements that are so wonderful lead to? And, as has been noted many times (even in this post!), dietary changes to control issues (T2 diabetes, high cholesterol, obesity), exercise, increased sleep are NOT alternative medicine; they are part of every good physician's care.
Followup post here:
http://scienceblogs.com/insolence/2016/06/24/the-mend-protocol-for-alzh…
Please move this comment thread over there. Thanks.
Want to find out what the "MEND protocol" is? Guess you have to buy the book..
"Dr. Bredesen’s book describing for a broad audience the interventions described in this paper, will be released by Penguin Random House in May 2017." (From http://www.buckinstitute.org/buck-news/reversal-memory-loss-ad).
It all sounds rather sketchy. Too bad. It is always hard to know what to make from what is essentially a case series, but it does sound like one or more of this group of interventions might of worked for some individuals. It is impossible to tell though from the way this thing was put together and all the unmentioned conflict of interests makes the whole thing sound very questionable.