
I don't know if you've seen any of the posts here at Scienceblogs or Panda's Thumb about the Discovery Institute's newest protégé, Dr. Michael Egnor. A professor of neurosurgery at SUNY-Stony Brook, Dr. Egnor has been pontificating on how "Darwinism" has nothing to offer to medicine; and indeed, that evolutionary biology has "hijacked" other fields of study. Mike has already aptly pointed out many of Egnor's strawmen and intellectual dishonesties, so I won't review them all. I've stayed out of the fray until now because I've had limited time and others have been handling it quite ably, but he keeps treading into (and butchering) my territory, so I just wanted to point out a few other things Egnor is waving away when he makes statements like this:
Preventing the emergence of resistant strains of bacteria is important work, but the insight that Darwinism brings to the problem -- the unkilled ones eventually outnumber the killed ones -- is of no help. We can figure that out ourselves. The tough work on preventing the emergence of resistant bacteria is done by microbiologists, epidemiologists, molecular geneticists, pharmacologists, and physicians who are infectious disease specialists. Darwinism, understood as the view that "chance and necessity" explains all biological complexity, plays no role.
Sigh.
Others have already addressed the blatant ignorance of this statement (spouted following a paragraph wherein he claims that the evolution of antibiotic resistance is just a tautology), so I'm actually going to leave the antibiotic resistance stuff alone for the time being. What I want to address instead are other areas where evolution is critical for insights into many of those fields Egnor mentions, especially since my own research is at the convergence of the first three he lists: microbiology, epidemiology, and molecular genetics.
Egnor has claimed in multiple posts (starting here) that "evolutionary biology contributes nothing to modern medicine," or even worse, that:
...it's safe to say that the only contribution evolution has made to modern medicine is to take it down the horrific road of eugenics, which brought forced sterilization and bodily harm to many thousands of Americans in the early 1900s. That's a contribution which has brought shame--not advance--to the medical field.
What's baffling is that Egnor is able to cite the fields he does above and somehow separate them from evolutionary biology. I'm not exactly sure how he thinks these differences in the "molecular genetics" in a population have come about, if not for "chance and necessity"* at the heart of things.
Phylogenetic analysis and evolution
For example, I've written previously about using the molecular data acquired from sequencing Ebola viruses in order to predict where the deadly virus may emerge next, using similar data to find the possible origin of HIV, or to to determine the source of a viral outbreak, as in the case of avian influenza in Nigeria. Here, they examined whether multiple outbreaks in an area are due to a single introduction event or multiple ones. In any phylogenetic analysis, we make certain assumptions, and (I'm simplifying this considerably) one of those is that closely related sequences reflect a more recent common ancestor. Therefore, the strains have *evolved* via "chance and necessity", accumulating mutations along the way that allow us to estimate the time of divergence from their most recent common ancestor. Now, one could certainly say, "well, I don't accept your assumptions," or "I believe your assumption is based on the false pretense that evolutionary theory is true," but then I hope they'd provide us with a better explanation for the results we obtain. "They were just designed that way" simply doesn't cut it; it doesn't give us a framework to analyze our results in any meaningful way, and it certainly doesn't contribute to an understanding of the spread of infection.
Other molecular genetics and evolution
And guess what? We use this assumption all the time in hospital epidemiology as well. Egnor glibly brushes off the significance of evolutionary biology to the problem of antibiotic resistance, so let's take another route. Imagine there's a bacterial outbreak in the hospital where he works; let's say, Legionella. We don't even have to make it resistant to antibiotics. 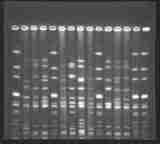 Epidemiologists will work to trace that outbreak to the source, be it a patient, a hospital worker, or an environmental source. (In the case of Legionella, a water source is often found to be contaminated). To investigate these outbreaks, molecular epidemiologists typically use a method called PFGE (pulsed-field gel electrophoresis). It works, essentially, by using a protein to chop up the DNA of the microbes and running those pieces of DNA out on a gel. The protein will cut at specific DNA signatures within the genome, and how many times it cuts (and therefore, the resulting number and size of the DNA pieces the investigator will see on the gel) is a reflection of the genetic makeup of the microbe. This is commonly referred to as its "DNA fingerprint" (see an example at the left). Again, the more similar results, the more recent a common ancestor between any two strains. Therefore, if we see the same "fingerprint" in the sickened patients and a shared exposure to a water source found to be contaminated with the bacterium, we can likely conclude that the water source is the origin of the outbreak. Evolutionary biology hasn't "co-opted" this analysis; rather, the analysis only makes sense with the assumption of common descent and subsequent divergence--aka, evolution. Egnor may claim that there's no "department of evolutionary biology" at his med school, but there sure as hell are people who use evolutionary theory right there in his hospital.
Epidemiologists will work to trace that outbreak to the source, be it a patient, a hospital worker, or an environmental source. (In the case of Legionella, a water source is often found to be contaminated). To investigate these outbreaks, molecular epidemiologists typically use a method called PFGE (pulsed-field gel electrophoresis). It works, essentially, by using a protein to chop up the DNA of the microbes and running those pieces of DNA out on a gel. The protein will cut at specific DNA signatures within the genome, and how many times it cuts (and therefore, the resulting number and size of the DNA pieces the investigator will see on the gel) is a reflection of the genetic makeup of the microbe. This is commonly referred to as its "DNA fingerprint" (see an example at the left). Again, the more similar results, the more recent a common ancestor between any two strains. Therefore, if we see the same "fingerprint" in the sickened patients and a shared exposure to a water source found to be contaminated with the bacterium, we can likely conclude that the water source is the origin of the outbreak. Evolutionary biology hasn't "co-opted" this analysis; rather, the analysis only makes sense with the assumption of common descent and subsequent divergence--aka, evolution. Egnor may claim that there's no "department of evolutionary biology" at his med school, but there sure as hell are people who use evolutionary theory right there in his hospital.
Vaccine design and use
In Egnor's initial post, he mentioned Jenner's invention of vaccines, which was carried out before Darwin was even born. And sure, this is true. Ancient peoples also performed crude brain surgeries before the dawn of modern medicine, but that doesn't mean that we haven't been informed and surgery improved using modern scientific evidence. What Egnor perhaps doesn't realize is that evolution impacts vaccination design and implementation in many different ways. The first is the design and formulation of the vaccines themselves. One common example of this is the influenza vaccine, which needs to be re-formulated every year because of the rapid evolution of that virus. Other vaccines sometimes contain only particular serotypes of the pathogen. For instance, the new HPV vaccine contains only 4 serotypes of virus: 6, 11, 16, and 18. We determine these virus types using molecular methods such as those mentioned above, but again, evolutionary theory underlies all of those results.
Additionally, especially for a vaccine that doesn't prevent infection with all types of a pathogen, we can't just throw a vaccine into the population without trying to understand how it will affect the rest of that pathogen species. For example, if we end up with a high level of herd immunity to the HPV serotypes mentioned above, does that mean other serotypes will replace them? Or even, potentially, unrelated organisms that previously occupied a similar niche, but were out-competed by the organism we're going to vaccinate for? We've seen this phenomenon (serotype replacement) with the pneumococcal vaccine already, and it needs to be considered and investigated with any vaccine of this nature.
Furthermore, we use evolutionary biology to investigate and predict not only what a vaccine may do to the ecology of a particular pathogen, but how it may affect the overall virulence of the population as well. (For instance, see this Nature article on "imperfect vaccines" and how they may contribute to the evolution of virulence--but I suppose that's just "citation chaff").
Who are the people who carry out this research? They are microbiologists, epidemiologists, molecular geneticists, pharmacologists, and physicians who are infectious disease specialists. And we all "hijack" evolutionary biology in order for our work to make sense.
------------------------------------------------------
*It should be noted, of course, that the "chance and necessity" characterization is really another of Egnor's strawmen. Sure, random mutations occur and sure, many times natural selection increases or decreases the prevalence of these mutants in the population, but sometimes these are either silent (and therefore are unlikely to be selected for or against) or simply don't register enough to be subject to selection in the current environment of the organism. However, they can still accumulate mutations, which we can measure via sequencing. Additionally, evolution in a population can occur even when "necessity" isn't involved, via a host of chance events. So I'd argue that "chance and/or necessity" would be better than just "chance and necessity" that Egnor provides. Of course, that makes it obvious that his argument is a strawman, so I suspect he wouldn't concede that point...
Image from http://www.cfsan.fda.gov/~dms/fsirp994.jpg
{kind=link}
thank you wery mach
Great work, though.. Thanks much!
Whilst his use of the term "Darwinism", attempts to conflate natural selection with eugenics, and so on do illustrate a remarkable silliness, I sometimes wonder if he (and other articulate creationists) are confusing implementation with theory. (I use "theory" in the proper sense, as a plausible testable refutable hypothesis.)
To illustrate by analogy: I'm a (software) engineer. Call me a programmer. One common programming task is to sort a list of things according to some metric. For instance, the letters:
B A E C D
would be, sorted by the usual alphabetical metric (A < B < …):
A B C D E
The implementation is the algorithm (computer code) used to achieve that result given that metric and that input. There are many possible implementations.
What a good programmer should do is simply use a pre-written implementation. Her or his task includes identifying a suitable implementation, using it, and testing it. However, she or he doesn't necessarily have to know how it works (the theory); what she or he is more interested in is whether or not its easy to use, small enough, fast enough, cost-effective, and so on.
(Better programmers avoid the need to sort, and not-so-good ones start by writing their own implementation of a sorting algorithm.)
Hence, the pre-written implementation user not only might not know the theory, but might believe it to be unimportant or even wrong. As long as the (results of using the) implementation is suitable, "who cares?".
But the implementer--dare I say designer?--of the sorting algorithm has to know the theory. (This is broadly true even if it's copied out of one of the standard reference works.) And has to know how to test and measure it. If it doesn't work, it's no good. And she or he needs to be able to say to the potential users, "it works best for so-and-so sized lists, uses such-and-so much memory and time, and ...".
The Ignors sometimes strike me as being like the "don't need to know the theory" algorithm-users, as opposed to the "must understand the theory" people who provide the algorithms.
Just a passing though...
Excellent point. Egnor only appreciates developments in biological science from the perspective as an "appliance operator", not as a developer himself. Thus he misses a lot of what went on behind the scenes to create the tools we use today. We can't see beyond the black box of Promega kits...
For gosh sakes, don't try to tell me that Lederberg's Nobel prize winning research into the nature of phage and bacterial genetic variation had nothing to do with evolutionary theory or had no impact on medicine.
Given that a number of individuals associated with the Discovery Institute are also HIV/AIDS deniers, in addition to being evolution deniers, it would be interesting to determine Dr. Egnors' views on this subject as well.
My biggest problem with the argument is that if resistance was designed into bacteria, then bacterial resistance would have been instantaneous and universal rather than slowly emerging, dependent on multiple parallel pathways of evolution to generate new resistance phenotypes, and distributed in disparate locations around the globe.
In other words, if there was a designer, antibiotics would never have worked because all the genes, including the resistance genes, would have to have existed all along. Unless god is still actively slipping in new genes along the way, this is a silly way to describe an emerging problem, that has found such a variation of ways to fight back against treatments. The Wiki on Beta Lactamase is interesting in this regard.
Superb article. so well written that a non-scientist like me can comprehend the points. Dr. Egnor has no excuse.
Maybe Egnor could appreciate the point he is missing from the standpoint of a farmer. After all, if a dumb, old farmer can understand something to be sure a famed neurosurgeon can understand the same thing.
When herbicides first appeared in the 1960's, there were only one or two and even as more developed, they tended to kill the weed in the same way. Of course, this is not good because in a few years you begin developing fields of resistent weeds.
Today's farmers have a rotation choice of eight classes pesticide, amino acid synthesis inhibitors, seedling growth inhibitors, growth regulators, photosynthesis inhibitors, lipid synthesis inhibitors, cell membrane disruptors, pigment inhibitors and a few whose mechanism is listed as unknown. However, in the early days, farmers still achieved a rotation by allowing a field with resistent weeds to lie fallow for 2-3 years, thereby allowing nonresistent weed stocks to increase and interbreed with resistent weed stocks. In annuals, this meant by Year 2 or Year 3, the vast majority of weeds were nonresistent where before they had been the vast majority resistent. The remaining weeds were able to be controlled by mechanical means.
Now if farmers in the 1950s and 1960s could figure this out, does this mean a worldclass neurosurgeon should be able to work out the same thing himself?
The synchronicity of the web - I just had the same idea, and posted comments here and here.
Egnor roughly says that we don't need evolution to tell us that resistant bacteria will survive and multiply and outnumber non-resistant bacteria.
We could do that. It wouldn't even be an ad hoc, but perhaps a robust theory against the observations he may want to do. Rather like Newton gravity (resistance) against general relativity (evolution).
First, here the simpler theory follows historically after the more general. So even if Egnor would be the Isaac Newton of resistance theory ;-), he would have nothing to be proud of.
Second and more seriously, the more constrained theory isn't robust against better theories. It is always replaced by the more general theory since the later has increased predictive power and ability to grow and connect with other theories. Egnor is confusing theory with model here. As bif discuss, it is when we model specific examples we may want to use the most constrained, simplest, model we possibly can find.
Perhaps this is why he haven't presented an alternative creationist theory like the frontloading theory. Not understanding the hallmark and importance of predictiveness in theories, not understanding the difference between modeling and theory - egnorance of science seems to be the trademark of Egnor.
Egnor writes
I think, Tara, that your article misses the mark because you fail to grasp that Egnor really is stupid enough to think that the work of evolutionary biologists (what Egnor IDiotically calls "Darwinists") rests on that strawman triviality. Regardless of how many times it is explained to Egnor what natural selection does mean, that it's about the distribution of alleles (which manifest as traits in the phenotype), he continues to repeat that idiocy or some variant of it.
After reading what Egnor has said over the past few weeks I am simply astounded that the Discovery Institute managed to find someone that says things that make them look even more idiotic than Dembski, Behe and Luskin did. Of course, this is all my opinion. Stupidity is, after all, in the eyes of the beholder.
Of some interest is a report on Rosenhouses' blog about an ID conference in Knoxville, Tn. Attached is a quote from Michael Behe, "Behe graciously clarified that some Darwinian claims are well-substantiated. Darwinism explains antibiotic resistance and certain genetic diseases, for example." It would appear that perhaps Dr. Egnor should consult with his Discovery Institute colleague on this matter. Of course, Behe also accepts common descent, which other Discovery Institute colleagues such as Casey Luskin reject.
While I agree with you, truthmachine, the article isn't written for Egnor. I've been doing this for quite awhile, and I'm very well aware that for many creationists, no amount of evidence, logic, or even common sense is going to strip them of the views they hold. I write for anyone who's on the fence or maybe just beginning to investigate intelligent design, thinking, "hey, this guy's an MD, his article sounds official, and he might be on to something."
Egnor will be convinced once he actually observes bacteria giving birth to cats and the extinction of PYGMIES + DWARFS.
One interesting point for me is that 'algorithm users', like farmers fighting insect pests, can use the results of evolutionary studies without understanding the theory. It shows how far evolution has moved beyond speculative theory into the realm of established fact. If you want to know what people really believe about evolution, watch a cotton farmer with a boll weevil problem, and see if he applies prayer or pesticides.
Speaking of insecticides, I once saw an insecticide-free way of get rid of soil critters before planting fields, simply by injecting steam into the soil, parboiling worms and parasites.
The documentary explicitely mentionned that insects were less likely to evolve resistance ... to superhot steam. Shows that even agri-documentaries are keenly aware of insecticide resistance, attributed to evolution.
I am glad to have the change to read all. Very useful information for all who has interest in this area. I personaly had great advantage from these informations.
very interesting artcile. Keep up your writing
Good idea! Best regards
like you
Like you.
I think you're missing the point of what Egnor might be saying. This is one thing that upsets me within the evolutionist-science sphere. They tell me what random selection 'means,' but they don't really see what it 'really' means. In other words, they may say that natural selection is 'random' because that's what it is, according to the scientific dictionary. But when we examine it more closely, especially from a philosophical standpoint, natural selection is not 'random' it has purpose : survival (one of others.) So, no matter how much you keep shouting 'no, it's random' that doesn't change the fact that it isn't. The words 'random' and 'chance' have different meanings in science to the normal english dictionary, and that is one of the main problems here (I think.) Science should use the words in comparison with the way the rest of the world uses those words, or rather find new words.