
It seems to me that the science of epidemiology is a lot like being in shoe sales in a country on the pacific rim. You never know when the other shoe is going to drop, but you know it will. Our species (humans) is numerous, contiguous, and dense (in more ways than one). This means that a highly virulent pathogen could spread across the globe and kill a gazillion people before we could do anything to stop it. Yet, such a thing has not happened in modern times, meaning, since the widespread and easy flux of population provided by the airline industry at several scales of space.
At the present time we (humans) are faced with yet another threat of pandemic disease, this time from the coronavirus MERS-CoV. Spoiler: It is very unlikely that MERS-CoV is going to be a major pandemic because it does not seem to be all that virulent, in the sense that it does not seem to spread easily from one person to another. When it shows up in a population, it does not seem to spread around quickly. On the other hand, it is human-spreadable, similar coronaviruses are virulent so maybe this one could evolve to be so, and the mortality rate is so far an alarming ~50%. And, there is another complication. MERS-CoV is very likely to be carried from its homeland in the Middle East to several other countries by the mass movement of pilgrims returning from The Haj.
A recent study in PLoS Currents Outbreaks (yes, that's a clumsy phrase, not a typo) looks at the situation. Researchers use reasonably good (but limited) data on air travel to estimate the number of people who will return-travel form the major Middle Eastern pilgrimage sites between June and November. They look at relative rates of return-travel to each area, and at health care expenditures per capita as a way of estimating the ability to address an influx of deadly disease-carrying return visitors, in each country.
16.8 million travelers on commercial flights departed Saudi Arabia, Jordan, Qatar and UAE for an international destination between June and November 2012. 7.5% had final destinations in countries that were low income, 47.4% lower-middle income, 17.3% upper-middle income and 27.8% high income. 51.6% had final destinations in just eight countries: India (16.3%), Egypt (10.4%), Pakistan (7.8%), the United Kingdom (4.3%), Kuwait (3.6%), Bangladesh (3.1%), Iran (3.1%) and Bahrain (2.9%; see Table). Individual cities with the highest travel volumes include Cairo, Kuwait City, London, Bahrain, Beirut, Mumbai, Dhaka, Karachi, Manila, Kozhikode, Istanbul and Jakarta, each of which received more than 350,000 commercial air travelers from MERS-CoV source countries between June and November 2012. Furthermore, an estimated 8.7% of foreign Hajj pilgrims in 2012 originated from countries that were low income, 56.4% lower-middle income, 27.3% upper-middle income, and 7.6% high income. 60.7% of foreign pilgrims originated from just eight countries – Indonesia (12.4%), India (10.1%), Pakistan (9.9%), Turkey (7.8%), Iran (6.5%), Nigeria (5.7%), Egypt (5.5%) and Bangladesh (2.9%). A bubble plot depicting the volume of international travelers departing Saudi Arabia, Jordan, Qatar and UAE from June to November 2012, the estimated number of foreign pilgrims performing the Hajj in 2012 and estimated healthcare expenditures per capita in 2011 is shown in Figure 1.
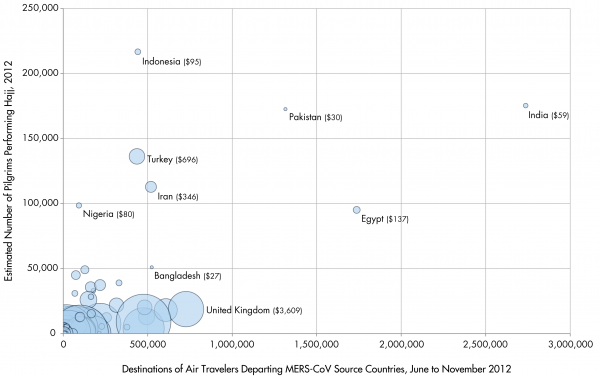 Fig. 1: Country-Level Destinations of Air Travelers Departing MERS-CoV Source Countries*, Origins of Hajj Pilgrims†, and Healthcare Expenditures per Capita‡
Fig. 1: Country-Level Destinations of Air Travelers Departing MERS-CoV Source Countries*, Origins of Hajj Pilgrims†, and Healthcare Expenditures per Capita‡* Final Destinations of Air Travelers Departing Saudi Arabia, Jordan, Qatar and the United Arab Emirates via Commercial Flights between June and November 2012† Estimated for 2012 ‡ Sizes of the circles are proportionate with healthcare expenditures per capita as estimated by the World Bank, 2011
The researchers note that MRS-CoV has the potential of being a pandemic disease, and that understating population movements that could underly its spread is essential. The key points here seems to be that there is an intersection between countries that have a lot of pilgrims returning from MERS-CoV source areas and a low probability of detecting and containing cases of international spread because of inadequate health care systems. Related to this, they also identify possible blind spots in the global health care industry. For example:
The four countries with confirmed cases in returning travelers...the United Kingdom, France, Italy and Tunisia...account for an estimated 7.1% of the final destinations of all international travelers departing the MERS-CoV source countries since September 2012 (each of which are high or upper-middle income countries). By comparison, India, Pakistan and Bangladesh represent the final destinations of an estimated 27.7% of all international travelers over the same time period (each of which are low or lower-middle income countries), but have not reported cases of MERS-Co. Although not definitive, these findings could indicate the presence of epidemiological “blind spots” to MERS-CoV as a result of limited infectious disease diagnostic and surveillance capacity.
So, we'll see how this goes.
Above I note that despite the obvious risk of a global pandemic of something spreading across the human population there really hasn't been one, but I think this should be put in context. We have had widespread and multi-layered (in terms of economic and other strata) air flight for less than fifty years, but that air travel has probably not penetrated all regions of the world until the last 25 years or so. Pandemics with really large death tolls, however, are very rare. The HIV/AIDS pandemic is a slower moving but very deadly one, and is the largest in modern times, and it started in 1981 and was certainly facilitated by the ability of humans to travel. The previous large pandemics that could possibly have been facilitated by air traffic in a major way were two flue pandemics, in 1968 and 1957, each very small compared to HIV/AIDS but effective at a much higher temporal rate. The previous pandemics that were very large, but prior to major air travel effects, most likely spread internationally with boat traffic, were the famous 1918 flu pandemic and the less famous 1889 flu pandemic, and a handful of near-million death level cholera pandemics, in 1899, 1881, and the 1850s.
So, during the 163 years from 1850, worldwide pandemics that killed 6 figures and above happened about 8 times. That's about every 20 years. So, when we look back at the history of air travel, which has allowed the ready movement of large numbers of people across a wide range of social and economic categories living in most populated areas, we should not be surprised at the number of pandemics. It is hard to put a year on when humans became as internationally mobile as they are today, but the east-west divide was a major factor dampening movement until the 1990s. One could say that the current highly mobile situation dates to about 1990, and is thus, just over 20 years long. In other words, the rough time scale of the emergence of diseases with the ability to spread widely and quickly, using cholera and flu as a proxy for "disease" is once every 20 years, and the situation in which the Giant Killer Pandemic in which human population is measurably reduced because of a disease we can't control for several years could occur is recent. I quickly add that Cholera is a lousy proxy for such disease because it is readily treated these days and its initiation and spread is only partly related to human movements. It may well be that the frequency of the evolution of a spreadable pandemic disease is much longer than 20 years.
There are shoes. They can drop. They seem to drop slowly, infrequently, but as time has passed over the last few decades the potential severity of such an event has clearly gone up in some ways while our ability to control disease through treatment and vaccination has probably stabilized or even gone down.
MERS-CoV is probably not the next pandemic. But the idea of there being such a pandemic, and even a pandemic with previously not seen qualities because of our denser than ever, larger than ever, and more connected than ever population is nothing to sneeze at.
________________________________
Khan, Kamran, Jennifer Sears, Vivian Wei Hu, John S Brownstein, Simon Hay, David Kossowsky, Rose Eckhardt, Tina Chim, Isha Berry, Isaac Bogoch, Martin Cetron. 2013. Potential for the International Spread of Middle East Respiratory Syndrome in Association with Mass Gatherings in Saudi Arabia. PLoS Curents Outbreaks. July 17, 2013. Full Text here.
This is my doomsday nightmare, and it's a broader cultural one as well, having replaced a broad US-USSR nuclear exchange as end-of-the-world material. What I find interesting is how the threat of mortality gets exaggerated in fictional versions of the pandemic. The worst pandemics in recorded history do not reduce broad populations by 50%: even the Black Death, the most infamous pandemic ever, had a net mortality in Europe of around 1/3. Science fiction pandemics generally look for mortailty rates around 90% like Ebola.
What level of mortality actually entails a noticeable level of societal collapse? Does mortailty affect the virus's global spreadability? Ebola's tendency to burn itself out suggests this. How realistic are the nightmares of Twelve Monkeys, 30 Days, that Wired Magazine scenario... all the nightmares that haunt me, in short?
All good questions. I tend to think that starvation plus disease is the nightmare scenario.
David Quammen does a good job, IMHO, with last years book Spillover in exploring the jump from animal world to human. We have been extremely lucky thus far, and you are right - we are waiting for the other shoe to drop.
@Minneapolis in the black death scenario it must be remembered that there was a much greater portion of the population that were, relatively speaking, much more self-sufficient than first world populations are today. Losing 30% of the population today could easily bring about the mass starvation Greg mentions, as transportation, storage and food production networks break down. A similarly virulent pestilence today will take out much more than 30% of the population in 1st world countries as well as the crowded cities of developing nations.
30%? Possibly way less. Every bite of food is at the end of a long supply line that is not set up to be redundant but is highly parallel. The market works very well with large swings in production, maybe up to that 30% range, in specific sectors. This year, British wheat is expected to be 20% off, which is a lot, but that's doable because somewhere else will surely be 20% up, and if wheat prices go up there will be minor adjustments here and there to use other materials where possible.
But in a situation where everything goes down 10% and nothing goes up, and there is simply 10% less food .... well, at first that might be covered with reducing the easy to reduce waste, but over a three or four years of a global decrease in that range (say 5 to 10%) and a continued increase in population there would be large areas of starvation. That, in turn, would make a large percentage of the population much more vulnerable to disease. Starvation kills a lot of people but it never really kills those people; a deficit of energy makes them vulnerable to things that don't normally kill.
Then, that in turn reduces the food supply because those people will be peasants in Thailand or whatever producing a big part of the world food supply . And so on.
Doom, we are.
The 2050 mark that is now being talked about for when supply will equal demand (peak food, as it were) is not so much the point where all the new babies grow up hungry from then on, but rather, when things like Arab Spring look like picnics.
Nat @1: Death rates from infectious disease of around 90% were reported in some of the native populations in early 17th century New England. Plimoth Plantation was founded on the site of a native village that had been abandoned due to an unspecified plague a few years before the Pilgrims arrived.
That was a special circumstance: the people of the Americas had been isolated from a number of diseases to which surviving Eurasians had largely acquired resistance, so they fell in great numbers when they finally encountered those diseases. So it may be unlikely today. But I would not call it impossible. And as others point out above, our modern interconnected world is likely to break down in a pandemic with a mortality rate well short of 90%.
Ebola and its relatives tend to burn out because they are too virulent. Afflicted individuals don't have much time to spread the virus to others before dying. But something that had a week or so for an incubation period before symptoms became apparent, and went on to kill a double-digit percentage of its victims, would be really nasty. Thanks to modern air travel, something like that could spread worldwide before anybody knew there was an epidemic.
Surely the percentage would not have to reach this level before serious problems hit: with almost immediate communication now wouldn't groups begin reacting badly by the time deaths hit 10%?