
UPDATE: The latest numbers do not indicate a weakening of the outbreak. (See list of new cases below. Several graphs have been updated as well)
UPDATE: More detailed discussion of transmission of Ebola
UPDATE: I note with sadness the death of my neighbor (though I did not know him) of Patrick Sawyer, of the Liberian Ministry of Finance, who died in Nigeria of Ebola contracted in Liberia. He was on his way home to Minnesota at the time.
There is an Ebola Outbreak currently underway in several West African countries, mainly Sierra Leone, Liberia, and Guinea. This is the most extreme known Ebola outbreak to date. The first known outbreak of this virus was in 1976, and there have been several instances since then ranging from single cases (which by definition are not outbreaks) to 425 confirmed cases (with 224 deaths in that instance, in Uganda, 2000-2001). The current outbreak is significantly larger with about double that number or more.
There is some confusion in the press (most notably in CNN) about the nature of Ebola and perhaps about some of the details of this outbreak. Here, I want to provide some basic data to help clear some of this up. CNN reported at one point that you can get Ebola only after a person is symptomatic, and (in the same story) at any time a person is infected even if they are not symptomatic. It is probably the case that as long as Ebola is in a person's system, they can spread it. It is only spread through contact with bodily fluids, but that is not such a hard thing to do; mucus membranes can absorb the virus, as well as cuts or other injuries. It is probably sexually transmittable. It does not appear to be airborne, but bodily fluids that are in or on needles, hospital equipment, etc. can carry the disease to another person.
Another issue with reporting is the difference between suspected cases, likely cases, and confirmed cases. Even within the health community these numbers are all over the place because they are always changing as cases go from suspected to either eliminated or confirmed. Wikipedia and CNN both recently stated that there have been 1,093 human cases with 660 deaths so far. However, this includes both confirmed and suspected cases. There is a good chance that the total number of cases is in fact close to this, but the data are of lower than ideal quality. If we want to look at mortality rates and changes over time in this outbreak, it is better to look at a smaller subset of the better confirmed data. That's what I'll do here. But, when looking at the numbers, keep in mind that although most of the data I show in graphics below show several hundred fewer cases than being widely reported, the actual number of people affected by the disease over the last four months or so is probably not only higher than the cleaned up data set but also, likely higher than the reported 1,093. Furthermore, the data I'm using here only go up to July 24th.
One of the most egregious errors at CNN is the frequent statement that Ebola has a 90% death rate, but that the current outbreak has a much lower death rate. This is rubbish. Ebola simply does not have a 90% mortality rate, and stating that the current outbreak is much lower in mortality gives the impression that this particular form of Ebola, or this particular outbreak of the disease, is somehow not as bad as usual. In fact, this outbreak is worse than any previous outbreak for several reasons. For one, it is larger. Also, it seems to be not burning itself out like most previous outbreaks did. Ebola outbreaks in the past have tended to happen in relatively isolated areas, because the population that includes victims is in close proximity to the presumed reservoir of the disease (probably fruit bats) and interacts directly with the intermediate hosts (eg. primates or other mammals that picked up the disease from fruit bats*). But there is plenty of reservoir and intermediate reservoir in some areas near major population areas. Apparently, Ebola broke into the human population in one or more areas of high population density, and this density together with relatively high mobility is allowing the disease to persist.
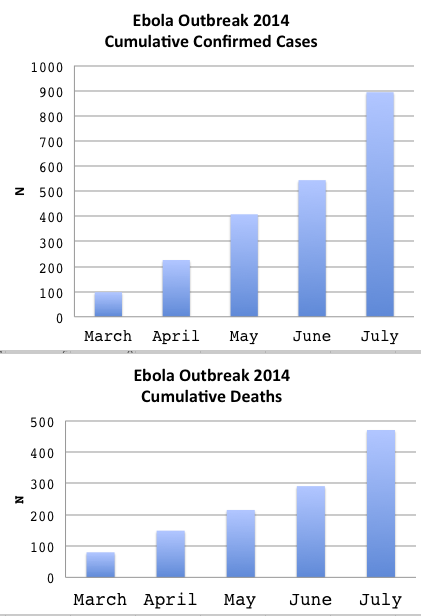
The following graphs are based on data I collected from the WHO reports. For March, I use only very likely cases, for April through July, I use only confirmed cases (not available for March). And, July does not include the last week for that month (a few more days have been added to this information bringing us to July 23rd, added on July 30th).
The following charts show the total number of cumulative cases conservatively estimated, and total number of cumulative deaths. When the outbreak starts to weaken, we would see a leveling off, but that is not indicated here (UPDATED).
The last several reports from WHO (including confirmed, probable, and suspect cases) are as follows:
July 21st through July 23rd: 108 NEW
July 18th through July 20th: 45
July 15th through July 17th: 67
July 13th through July 14th: 18
July 08th through July 12th: 85
July 06th through July 08th: 44
July 03rd through July 06th: 50
The exact time spans for each of these reports may not be the same, but I believe the number of cases do not overlap; each listing is a separate set of new cases. Clearly, for the last several days of available information, there is variation in, but no let up in, the number of new cases.
Looking at the number of new cases reported (and for the most part confirmed) and the number of deaths (the same data as used to make the cumulative graphic above, but by month) we have this (Updated):
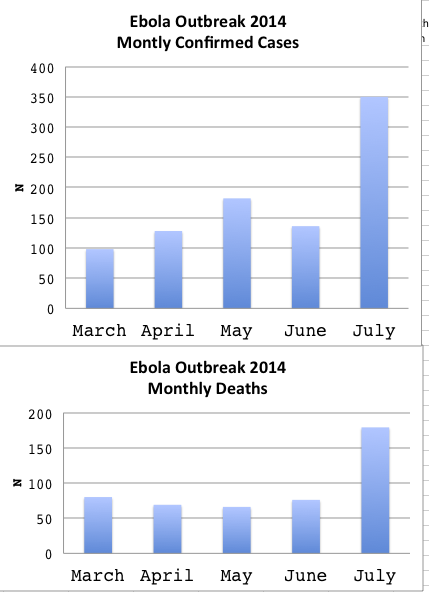
Keep in mind that the data for July are short by several days.
Another area where MSM, and for that matter, Wikipedia, could do a better job is in reporting the mortality rate for the disease. Wikipedia states that "The disease has a high death rate: often between 50% and 90%." This is misleading because the outbreaks with 90% mortality rates are not typical, and the statement seems to be based on a set of data that includes a lot of data points one would do better to ignore. I assume CNN is taking this information (from Wikipedia or elsewhere, which perhaps repeats the Wikipedia claim) and exaggerating slightly when they say that Ebola normally has a 90% mortality rate.
The Ebola affecting people right now in Africa is one of a handful of similar viruses known over a larger geographical range. Some of the deaths found in the larger data set of all known outbreaks are from individuals who showed up in a hospital nowhere near where they got the disease, or laboratory workers. The best way to estimate mortality rates related to the present outbreak in West Africa is to take only field cases -- actual outbreaks in normal populations -- in Africa only, and to not count "outbreaks" that are not outbreaks because only one person is in the sample.
The following chart compares mortality rates for all of the "outbreaks" listed in Wikipedia page regardless of size of sample, geography, or circumstances, with only those that are African Ebola in the field. The latter set also excludes the present outbreak.
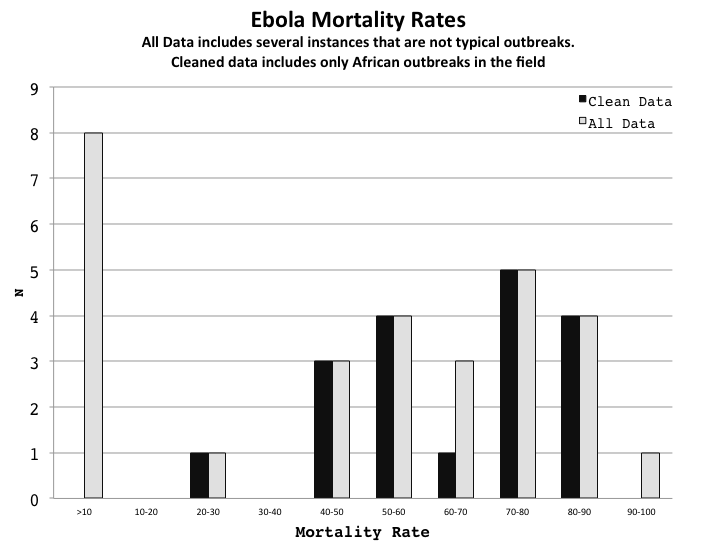
Notice that the clean data are bimodal; some outbreaks have mortality rates between 0 and 90%, others between 40 and 60%, and not much in between. Also, there are several in the all-data set that have a mortality rate of zero. This bimodality is not necessarily a persistent statistical characteristic of the sample; I could make it go away by changing the histogram intervals. But it is a convenient place to break the sample into "more severe" and "less severe" outbreaks.
The zero cases in the full data set are all odd cases. Seven are not in Africa and include in some cases lab workers or animal handlers, and most are not African (Zaire type) Ebola. One is a scientist who caught the disease from doing a necropsy on a chimp in the Ivory Coast, examining an outbreak among the non-human primates there. There is one case where the fatality rate is 100%, but this was only one person, and the case was discovered post hoc. We don't know if anyone else there had the disease. A 90% mortality rate occurred in a remote part of the Congo, with 143 people affected including health care workers. It appears that several individuals contracted the disease butchering non-human primates. This occurred during suboptimal conditions during the Second Congo War. One case of 88% mortality occurred early on in the history of the disease (the second known outbreak) also under very poor conditions. Although the data are too sparse to draw firm conclusions, it seems that the more severe outbreaks in terms of mortality tend to have occurred under more difficult conditions.
Ebola probably has a very high mortality rate when an infected person gets no medical treatment, and a mortality rate closer to 50% when a person quickly gets medical attention. There is no cure, but when a patient is given IV solutions in a hospital setting the chance of survival goes way up. This might suggest that smaller outbreaks that run their course before intervention would have a higher mortality rate, or that the mortality rate would be higher near the beginning of the event. Similarly, one might expect mortality rates to be higher in the early years of Ebola than later, as treatment methods developed.
There is some, but not much, evidence for these effects.
The following chart shows mortality over size of the outbreak, using only the cleaned up data set:
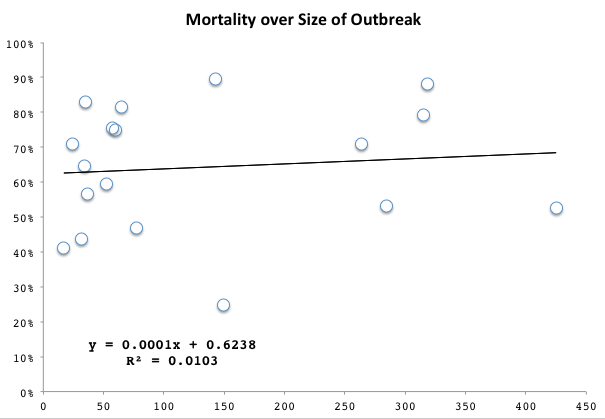
There is not a relationship between size of outbreak and mortality rate.
This chart shows the mortality rate over time, for the cleaned up data:
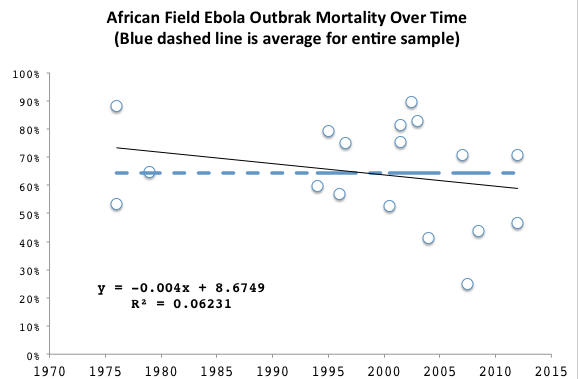
This seems to show that lower mortality has been achieved in recent outbreaks, though the statistical significance of this is non existent. But, the data set is small. The above chart also indicates the average morality rate across all of these events, which is 64% across 18 outbreaks. Not "usually 90%" as CNN states.
The following chart shows the approximate mortality rate for the current outbreak by month.

This is calculated from confirmed or highly likely cases. This is not a true mortality rate because people who got the disease in one month may have died the next month. But it does give an approximate indication of change over time in rates. The rate at the beginning of the outbreak could be high, or this large percentage could be a function of how cases were counted. In any event, this is an indication of higher mortality rates calculated at the beginning of an outbreak, and there are likely two reasons for that high rate, either or both applying in a particular case.
The current outbreak is settling in at about 60% mortality rate. There is no indication from WHO that the epidemic is slowing down.
UPDATE: Is Ebola Only Transmitted By Symptomatic Individuals?
According to the usual sources (WHO and CDC for example) the following is probably true. When someone gets Ebola, typically, after a while they get sick. This means they show symptoms. If they did not show symptoms they would not be “sick” even if the virus was in them and even if the virus is multiplying in them. Presumably people are infected with a sufficient number of viroids that they become a host for the disease, the virus starts to multiply above some level that makes the person sick, and we can say at that point that they “have Ebola.” This is when the infected person is able to transmit the disease to others through bodily fluids that might come into contact with wounds or mucous surfaces in the downstream patient.
This is what the WHO and CDC literature on Ebola says, and this has lead bloggers and news outlets to state incorrectly that Ebola is only transmitted to others when the person shows symptoms. Unfortunately this is not true in one or possibly two ways.
It appears that people who have had Ebola, live, and get “better” (i.e., their symptoms go away) can still carry Ebola for a period of time, and in this state, they can still transmit it. What has probably happened is their immune system has started to fight the virus enough that it is attenuated in its effects, but it isn’t’ entirely gone yet. Medical personnel like to send someone home only after the virus has cleared. Even so, men who are supposedly virus free by that standard, when sent home after surviving Ebola, are told to avoid sex for several weeks because there is still the possibility of sexual transmission of the virus. Meaning, of course, that the virus is still knocking around in some individuals at this point, and still transmittable. It is not clear how likely that is to happen.
This is very important. Most people would interpret “only transmitted by people showing symptoms” (or words to that effect) when they read it in a news outlet as meaning – well, as meaning exactly what it says. But post-symptomatic patients may still transmit the disease.
Is it possible that pre-symptomatic people can transmit the disease too? Personally I think it is possible even if it is generally unlikely. In a disease that kills over half of those who get it, “unlikely” is not comforting. A small percentage of people who never seemed to have had Ebola, or to have been exposed to it, seem to have antibodies that would probably only develop if exposed to Ebola. Some studies have shown immune reactions to Ebola in those known to have been exposed but also known to not have gotten sick. This is important but not shocking. There are a number of different situations where a normally icky disease that makes you really sick seems to have infected a certain percentage of people asymptomatically. Are these people carriers at some point, i.e., people who have the virus in them, can transmit it to others, but don’t get sick themselves? There is no evidence to suggest that this is the case with Ebola, but the total number of known human cases of Ebola is very small and the conditions for study of the disease in the field very poor, so the safest thing to conclude is that we simply don’t know, but it is also reasonable to say that asymptomatic carriers don’t seem to be a problem, or this would likely be noticed.
The important point here is that there is not a perfect correspondence to being infected and having symptoms, and transmission post-treatment and survival is possible and of sufficient concern that WHO and CDC assume it, so it would be unwise to make too many assumptions about pre-symptomatic transmission.
Imagine you are a health care person addressing an Ebola epidemic. An jet liner flies over a very long flight, say 10 hours long, on Monday. On Friday five people who were on the plane come down with Ebola and you have reason to believe that they were all infected before the flight. Would you determine that it was impossible for the nearly 300 people stuck on a tube with five pre-symptomatic Ebola carriers to become infected? No. You would watch those people and test them.
An additional point to underscore; it has been touched on but not emphasized. The symptoms of Ebola include vomiting and bleeding from places one normally does not bleed. Put another way, the symptoms of Ebola include spreading around bodily fluids. This is often how diseases spread. The disease results in a bodily reaction that spreads the disease (look up “virulence”). So, no matter what, the most likely transmission by far is during the period of symptomatic reaction to the disease, or for some time after death while the virus is still viable. That does not mean that there is no transmission before or after, but it does mean that the most obvious transmission will be from symptomatic patients or recently diseased symptomatic patients.
_______________
* Fruit bats will drop fragments, or stones, of fruit they feed on, sometimes in discrete piles. It is almost impossible to imagine a ground dwelling frugivore, such as a chimp or a duiker, not stopping to munch on this detritus. Since Ebola is spread through bodily fluid contact and can be spread via mucous membranes, and fruit bat spit counts as a bodily fluid, I'm personally of the opinion that this is how Ebola may often transfer from its natural reservoir, where it seems to exist without harm, to other animals. Of course, I figured this out after having discovered and handled several such piles of fruit bad wadge.
Could the bi-modal mortality rates be due to different strains of Ebola having different mortality rates? Maybe that's something that's already been investigated.
Also, does surviving Ebola give the survivor immunity?
There is no strong evidence I know of for different African Ebola to have that difference. There may be too many confounding factors to see that.
A number of Ebola survivors may have immunity but is they do or the level if protection is not known. There are indicators that they wold. Also some people never seemed to have the disease yet they have indicators of immunity.
Most viruses do have different strains, so it would not be surprising if Ebola did as well. According to The Hot Zone, a book written in the early 1990s on this subject, there are (or were) four known strains of Ebola, including Marburg (the first such virus discovered, named after the city in Germany where the index case, an animal worker, lived), Reston (named after the DC suburb, and the primary focus of the book), and two named after African countries. The Reston strain apparently did become transmissible by air; the good news there is that other mutations seem to have rendered it no worse in humans than an ordinary cold. Death rates for the other three, after hospitalization (it's likely many victims never made it to a hospital), ranged from 25% for Marburg to 90% for one of the African strains (the other was around 50%).
What makes this Ebola outbreak worrisome, as Greg mentions in the post, is that it is occurring in major population centers in West Africa. This makes it that much more likely that an infected individual will find his way onto a plane and spread the disease to somewhere else. Once you are in a city with an international airport, you can reach any other such city in the world, as well as much of the countryside around those cities, within 48 hours.
Right; the data I use for all of this except one series on one graph is African Ebola only. Which, probably, is internally fairly homogeneous in its effects insofar as one can see with samples small enough to make most epidemiologists cringe. The other forms are very different in mortality rate, etc. With the African natural Ebola there seems to be two main strains but strains is probably straining the meaning of strains; the finer genetic differences may be more important. There is a fair amount of variation.
At least one person, I think, did in fact fly somewhere then was found to be very sick thereafter. Short flight, though. Then again nobody enters the hospital room of a patient without wearing a mask.
There are five identified Ebola strains currently. The one causing this epidemic is Zaire Ebolavirus, the same one (roughly) that caused the original epidemic in 1976 in Zaire, and the one with highest virulence. Somehow it made it's way from there to West Africa, most likely in a bat host.
The other reason I've seen given for the size of this epidemic is the better road system and greater mobility of the W. African population, which makes sense if you look at the initial spread from pattern from rural Guinea to the capitol on the other side of the country.
If you work in R, I wrote a data scraper to compile data from the WHO GRN periodic reports, for cases and deaths:
http://ecologicallyoriented.wordpress.com/2014/07/13/ebola-epidemiology…
and 3 other posts on the topic.
Marburg is not considered an Ebolavirus strain, but a different virus in the same family (Rotavirus). It's highly lethal in the right conditions, equal to Zaire EBV, as demonstrated by outbreaks in the Congo and/or Uganda in the last couple of decades.
Nice r script!
I just updated the post, including adding a graph of the recent mortality rate. Note that the recent downturn therein (smoothed values) is not accompanied by same for the case rate, which is still climbing.
Correction: Filovirus family for EBV and Marburg, not Rotavirus.
There are possibly three (or more) things that could account for waviness in the death rate.
1) They get better at saving people, or more exactly, at getting people into the setting they use to reduce mortality. This is not one simple outbreak; there are many geographical localities involved. As a couple of new localities are hit, we might expect a higher mortality rate, as that locality matures wrt addressing the issue, we might expect a downswing. So, that would involve a tug on the line in both directions across time.
2) The number of "cases" that is used to determine the mortality rate is counted differently across time and space. There is controversy, for example, in one are where one agency is saying a number about 30% or so different from WHO. There could be some sort of moving bias on that. In general I would expect this to usually cause an upswing in death rate where case counts are older and thus more refined.
3) I would expect the end (present moment) of the curve to always curl down just because there are new cases where the people will die but have not done so yet. Edge effect.
I think 96 new cases but only 7 deaths is the biggest inter-report discrepancy between the two metrics I've seen yet. Potentially very serious.
I hope the drop in recent deaths is reflective of your point #1 (quicker and better care), but given what I've read about how the rural people in Sierra Leone are reacting to the medical and political authorities (fear, hiding, etc), I fear there are cases and deaths going unreported and that these are actually just minimum estimates that could be well off.
The other point about the fluctuations is the natural component--everybody thought the initial case/death upsurge in Feb/March had run it's course given the declining April numbers, and then, wham, the May-July numbers skyrocketed. We have no idea what's going on in the bat reservoir as far as I know, and now no idea on how many humans are actually infected.
It is a pretty bad situation.
I doubt the bats matter here. I suspect this is all human to human spread. But there could be something going on with multiple entry points related to bats and/or intermediate reservoirs.
What is the best current estimate of the basic reproductive number of the Ebola virus?
Considering that the current outbreak is equal in magnitude to several of the previous outbreaks, and infection is so closely tied to malleable behavior, I would not be surprised if this changes, but I believe it is 1-4
Call Dustin Hoffman, Rene Russo, Morgan Freeman, Cuba, Kevin Spacey and Donald Sutherland!
Well contact by bodily fluids is like hep B, Certainly something to on one's guard against, but not as bad as an air-born virus. Given that i am a little surprised at how fast it is spreading.
The CDC is still saying that Ebola is not transmitted from infected but still asymptomatic people. Is there any evidence to suggest that they should re-evaluate this statement?
Sad news: Dr. Sheik Umar Khan, Sierra Leone's top specialist in Ebola and hemorrhagic fever diseases, died of Ebola after treating more than 100 patients. In all likelihood, he was exposed while treating a patient.
There are reports in various news sites describing Dr. Khan and his life's work. The world has lost a great man, a brave man, a good man.
---
Greg, your article here is the best I've seen for solid facts about the outbreak.
Yesterday there was an interview on Public Radio with a physician who had been in Africa treating patients, and it was mentioned that American public health experts are starting to get more than slightly worried that this is going to start spreading to other continents. Have you heard anything along those lines?
Greg are you a science professor, geek (no offence intended) or some type of scientist? Just stumbled across your blog and wonder what are your qualifications? I am a recently retired teacher who loves science and has a basic working knowledge in this field. I am of the opinion that this current outbreak will indeed spread to other continents including Europe and the US. The only good thing is I believe the US may be better prepared to deal with a outbreak if it is contained. I also understand the need to not cause panic, but educating yourself now is key. Thanks for this post!
Cat, my About page has details. I'm a scientist and a writer. I actually informally worked on a small part of the Ebola problem years ago, supplying info and thinking to those working on the reservoir. I may or may not have contributed to our current thinking on where it normally lives and how it gets eventually to humans.
Remember, and I don't mean to seem callous, but in these very countries where over 1000 have become very sick, over half dead, at the same time orders of magnitude more have been stricken by malaria and other infections. Ebola is truly horrible and this outbreak is serious but it is a small public health problem, when it isn't happening! (That is probably why there is not a vaccine or treatment)
Ed, if you read everything the CDC says there is no contradiction with what I am saying. Same with WHO. I think there might be a problem with messaging, but this might be a larger problem than just Ebola.
G, thanks.
Ebola can go many days without detection, so getting out has always been a possibility. But the reservoir won't get out. It would truly be a flash in the pan. Ebola and related viruses have actually gotten out before, technically!
By the way, regarding getting out .... The man who sadly died in Nigeria, on his way elsewhere from Liberia, was on his way to his family in the US. Turns out he's my neighbor. I did not know him personally.
I would be curious to read more about the testing done on those potentially exposed to Ebola but considered asymptomatic. What is the test , how long does it take, how accurate is the test, and how soon after potential exposure will the test provide accurate results. Understanding this would go a very long way in reducing an increasing and understandable angst surrounding the whole, ''but what if someone does slip through" scenario.
Gary, there are several different things going on here.
Earlier and I think also very recent studies showed a background of prior infection I assume using standard virology techniques, looking for antibodies specific to Ebola. See:
http://www.nytimes.com/2000/06/27/world/people-carrying-ebola-in-some-c…
http://www.itg.be/internet/ebola/ebola-34.htm
http://jid.oxfordjournals.org/content/179/Supplement_1/S192.full
In addition people with recent exposure such as family members caring for those infected were repeatedly tested in at least one study to see what was going on with them, and interesting things were learned. See:
http://www.jwatch.org/id200007200000007/2000/07/20/asymptomatic-ebola-i…
http://onlinelibrary.wiley.com/enhanced/doi/10.1046/j.1365-2249.2001.01…
There was a good item on the Aussie ABC news on this here :
http://www.abc.net.au/news/2014-07-30/ebola-virus-explainer/5635028
I think.
One scary virus indeed - I first heard of this back at university where I'd wait for the bus at a bookshop and stumbled on Richard Preston's 'The Hot Zone' book on it - and ended up missing several buses! (Did eventually buy my copy from there.)
For a virus with this case fatality rate to spread this widely in a modern setting, I would guess it must have some risk of asymptomatic transmission and/or a mild version that is contagious, has a malaria/flu differential diagnosis but doesn't kill. Ebola has always burnt out and been contained easily in the past, and although the scale of this outbreak could just be bad luck, the multiple entry points and sustained incubation suggests something different.
The use of confirmed cases to calculate the cfr could therefore be very misleading. If it has a mild manifestation then the confirmed cases will be a severe undercount, and in this case could significantly hamper containment efforts. To compare with Spanish flu, that disease had a cfr between 2 and 20% from memory, but it's non-fatal manifestations helped it spread. If the cfr for this outbreak is even half that reported, and mild cases occur only occasionally, or the infectious asymptomatic stage is only a day or two, it is still the scariest disease in 100 years!
What about transmission via cough and sneeze? It seems to me that if the virus can be absorbed by mucous membranes, all it would take for transmission to occur via cough or sneeze is for an individual to be within proximity of that cough and sneeze and to have taken in some of the liquid from the infected person. I read that the CDC defines direct contact as being less than 3 feet in close conversation with an individual. There are other things they defined as direct contact but that prompted me to think that it is possible that bodily fluids could be exchanged even when two individuals are 3 feet away from each other. Does anyone have any opinions on this?
Aerosols produced from bodily fluids are dangerous places for viruses. In order for a virus to survive in that state they need to have certain features. Viruses that "spread through the air" have these features, and may also be able to survive on surfaces.
Ebola does not have those features. This is why by some (possibly confusing) terminology Ebola is not contagious even if is transmittable.
If, however, an infected individual coughed up a loogy (sp?) and it landed on someone's mucous tissue or open wound, the virus could pass safely to the next person. Beyond one meter (3 feet) loogies are rare, and projectile vomiting usually does not go that far or at least only hits your CDC approved boots.
Have just updated my post to include new numbers as of yesterday's WHO update, and with some substantial code modfications as well:
http://ecologicallyoriented.wordpress.com/2014/07/13/ebola-epidemiology…
I think the most likely explanation for the bimodality is simply that Zaire Ebolavirus (ZEBOV) is more virulent than the four other strains/species. All of the Zaire Ebolavirus outbreaks have had mortality rates in the 80-90 range. The other major outbreaks have been mostly Sudan Ebolavirus, (SEBOV) and the rates for that strain have typically been in the 40-60% range, even though the conditions of remoteness and available care have been roughly the same as in most of the ZEBOV outbreaks, the exception being this one. Ditto for a third strain that exists in the Uganda/Sudan region. The mortality rate of this one is about 61% now, but likely to rise because there are many now infected who have not yet died, and it appears that many are refusing treatment in clinics out of fear.
Jim, you should put your r cod here: http://www.r-bloggers.com
Different strains could certainly explain the mortality bimodality.
I used to live in northern Liberia, near the initial outbreak of the disease in Guinea. There's plenty of daily traffic from where I lived down to the capital in Monrovia. It wouldn't take much for the virus to get there from northern Liberia. And it's just a jump across the border to southeastern Guinea, with lots of tribal associations and families spanning both sides, meaning plenty of traffic there, too. And people travel those distances packed into small vans
...and covered pickup trucks. Plenty of close contact. And Sierra Leone is only about 40 miles farther west. Again, once the virus makes the short and easy hop across the border into Sierra Leone it's pretty much guaranteed to move towards Freetown because that's the direction traffic flows in Sierra Leone. So, to some extent, it was just bad luck that the virus popped up there, right at a place where three countries converge, each with their own transport systems pointing to three different widely separated national capitals.
Does anyone know if an infected individual survives, they would presumably now have antibodies. Are they nowprotected from getting the virus again?
That is probably true, Kristen. They do have antibodies, based on prior research, and we can guess that they would have some protection, maybe a lot of protection.
Greg,
I got *severely* bogged down and therefore not fully able to get to this, but since I promised, here are a few refs discussing the possibility of non-contact transmission of EBV. I agree that non-contact transmission is minor at best, compared to direct contact, but my point is simply that it should not be completely ruled out, which I am still not sure whether you are, or are not, doing so.
Gatherer, 2014, (in press). The 2014 Ebola virus disease outbreak in west Africa, lines 185-198
http://vir.sgmjournals.org/content/early/2014/05/01/vir.0.067199-0.short
WHO RISK ASSESSMENT, Human infections with Zaïre Ebolavirus in West Africa, 24 June 2014.
pg 4, "Evidence of human-to-human transmission"
http://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&…
Roels etal 1999. Ebola hemorrhagic fever, Kikwit, Democratic Republic of the Congo, 1995: risk factors for patients without a reported exposure
http://jid.oxfordjournals.org/content/179/Supplement_1/S92.full
Bausch etal 2007. Assessment of the Risk of Ebola Virus Transmission from Bodily Fluids and Fomites
http://nihbrp.com/Citations/completed/HumanHealthEcologyTeam/IssueBrief…
First paragraph of discussion section regarding live virus in saliva
Dowell etal 1999. Transmission of Ebola Hemorrhagic Fever, A Study of Risk Factors in Family Members, Kikwit, Democratic Republic of the Congo, 1995
http://jid.oxfordjournals.org/content/179/Supplement_1/S87.long
Table 2: "Exposures during late illness: Conversation"
(This paper's results are very confusing if you look closely at the tables, but nonetheless appear to provide strong evidence against non-contact transmission).
Jim
Jim
I've seen those studies/reports. Note that in the case where Ebola is identified in tissue types, there was a single example of Ebola in saliva. There are two studies here that suggest that we should be concerned about airborne transmission, the others rule it out.
Bausch et al 2007 says:
"Of particular concern is the frequent presence of EBOV in saliva early during the course of disease, where it could be transmitted to others through inti- mate contact and from sharing food, especially given the cus- tom, in many parts of Africa, of eating with the hands from a common plate. However, the isolation of EBOV from only 1 saliva specimen, in contrast to the 8 that were RT-PCR positive, could suggest that the virus is rapidly inactivated by salivary enzymes or other factors in the oral cavity that are unfavorable to virus persistence and replication."
This is interesting because airborne transmission may have been seen in pig to macaque and macaque to macaque. Bausch et al 2007 may be an indication as to why we don't seem to see airborne transmission in humans; something about human saliva. By the way, human saliva may be richer in certain enzymes than primate saliva generally, and variation across the components of saliva may relate to dietary adaptations, so this is not too surprising. Anyway, the relevant conclusion here is probably that even though Ebola appears in Saliva it is also killed there.
The other study with a suggestion of airborne transmission is the empirical study of infected patients by Roels Et Al (2014) which identifies a number (a small but not at all insignificant percentage) of apparently infected individuals who did not have direct contact with an ill person. This study is in contrast to a handful of other studies (one of which you cite) that seem to show no indirect contact transmission, and with the field observations of health care workers. Yet it is worth looking at. The problem is the quality of the data may be very low. From the study:
"Our investigation had several limitations. First, the team frequently had to rely on surrogates to provide answers for patients who had died. Responses by surrogates describing the type of contact between deceased patients and ill persons visited by the patient may have been inaccurate, particularly if the surrogate had not accompanied the patient. Second, the interviewers may have been more aggressive in attempting to establish potential contacts or risk factors for patients than for control subjects. Third, although serologic confirmation of all cases would have been preferable, only 11 of 44 cases provided sera for confirmation. Fourth, the interval between the period of interest and the date of the interview was long and may have resulted in inaccuracies. Fifth, our matched design made it impossible to identify specific risk factors during hospitalization or during a visit to a sick person.
In conclusion, we identified an exposure source for 32 of 44 patients for whom no source was originally reported. Of the 12 patients who did not have an identified exposure source, no sociologic, occupational, or dietary risk factors for illness were found. Direct person-to-person contact was the likely mode of transmission for most EHF cases during this outbreak. However, our findings suggest that other EHF transmission modes cannot be excluded and may account for infection in those individuals for whom no previously recognized mode of transmission could be documented."
If I was working on this I'd be trying to characterize saliva vis-a-vis Ebola survival. I'd be concerned that some subset of people have more Ebola-friendly saliva, or at least, I'd like to try to rule that out!
I'd also like to see any studies or data of any kind regarding decay rates for viral integrity/infectiousness as a function of time outside of a body. Certainly such data must exist, and could go a long ways toward determining transmissivity without direct contact. In other words, is it the lack of infectious virions in the lungs, throat and mouth that limits airborne transmission, or the stability of the virus, or some combination of the two?
Does anyone have the specific R0 data for the 3 African strains of Ebola (Zaire, Sudan, & Bundibugyo)? I can't find that data anywhere.
Also, understandably the mortality rates at the beginning of an epidemic will be inflated and then decrease with proper medical care. Any speculation as to why the mortality rate seems to be increasing again so significantly aside from the expected spread of the disease? Is the R0 changing? Are more people coming "out of hiding" so to speak and seeking aide?
Finally, according to the Public Health Agency of Canada, there is some belief that Ebola can indeed be spread via aerosols, this is the first I have heard of this but seemingly with the infective nature of this viroid that is feasible (full site here:http://www.phac-aspc.gc.ca/lab-bio/res/psds-ftss/ebola-eng.php). Has that been 100% disproven anywhere to date?
The statements on the Canadian site are at odds with WHO and CDC, but overlap with some real info; the monkey and pig cases are irrelevant to the human cases. There really is no evidence of a truly aerosolized version of the virus in the African outbreaks.
The mortality rate for this outbreak is not going up. The most recent report has a high rate (74%) but the average over the last month is close to 50. Don't put any weight on one report's rate.
Is there lifetime immunity to this virus? Does the virus mutate?
All viruses mutate, but getting Ebola probably gives you an immunity to Ebola.
Figures from a study by the Lancet in 2000 suggest there may be 1 patient with Ebola who remains asymptomatic for approximately every 10 patients who have symptoms. These patients appear to have low viral loads and so are likely to be less infectious to others, but their impact should be considered.
http://www.thelancet.com/pdfs/journals/lancet/PIIS0140673600024053.pdf
Stephen, yes, that is interesting.
Has there been a recent comment on the progress (or lack of progress) toward gettings slowed down in the hardest hit regions of Africa?
Greg, this more recent article in the Lancet suggests that these asymptomatic patients are perhaps the first good news we have heard about Ebola. Their presence is likely to slow down the spread of Ebola, and if identified by testing then they are a potential source of health workers who would not be in danger of becoming unwell from Ebola. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)61839…
i personally, have been reading strongly about this african ebola and wondering exactly how it so fast it is spread and how so fast can it be contained. pliz help and update me.