
I'm sure it's obvious that I'm often puzzled (and, I daresay, many other skeptics and boosters of science- and evidence-based medicine are puzzled too) over why various forms of quackery and woo that have either about as close to zero prior probability as one can imagine and/or (more frequently "and") have failed to show evidence of any therapeutic effect greater than that of placebo in clinical trials manage to retain so much traction among the public. Examples abound, for instance homeopathy and reiki, the former of which is nothing more than sympathetic magic prettied up with science-y sounding terms and the latter of which is nothing more than faith healing given a New Age mystic slant based on Eastern mysticism and religion rather than Christianity. Indeed, reiki was even inspired by stories of Jesus' healing powers, complete with a trip into the wilderness for fasting and prayer, resulting in revelation. Another example is acupuncture, a modality that is seemingly more popular than ever, even invading the very sanctum sanctorum of the ivory towers of academic medicine and the hard-nosed halls of military hospitals, yet every study of which that is done under rigorous conditions with proper placebo controls shows it to be no more efficacious than a placebo. It's easy enough to shake one's head and chalk it all up to irrationality, ignorance of science, or even religious faith. However, I've always been dissatisfied with such glib explanations, even though admittedly I have myself used them on occasion--or even to what I like to refer to as "burnin' stupid."
That's why a study released last week in PLoS One by Mark M. Tanaka, Jeremy R. Kendal, Kevin N. Laland out of the Evolution & Ecology Research Centre, School of Biotechnology & Biomolecular Sciences, University of New South Wales, the Department of Anthropology, University of Durham, and the School of Biology, University of St Andrews, Fife, respectively, entitled From Traditional Medicine to Witchcraft: Why Medical Treatments Are Not Always Efficacious. Besides loving the title, I also like the methodology, which in essence adapts the tools of modeling evolution and the spread of traits throughout a population and asks the question: Why do ineffective or even harmful (or, as the authors characterize them, "maladaptive") treatments for various illnesses and conditions persist in human populations? The results that the model shows are surprising and counterintuitive, yet to me they ring true. In essence, the authors show, using (mostly) reasonable assumptions that the most efficacious self-treatments are not always the ones that spread through a population and that even harmful treatments can spread. Both of these observations are entirely plausible based on the prevalence of usage of common woo and quackery, and what the authors have done, in essence, is to model mathematically why quackery persists.
First, the authors set the stage:
In recent years, 60-80% of the world's population, mainly from developing countries, depended primarily on traditional medicines, folk remedies and home cures, as well as treatment from witchdoctors and other 'supernatural practices', for their health-care needs [1]. In western societies, complementary and alternative medicine is garnering increasing interest and acceptance. At current growth rates, two-thirds of Americans are projected to be using alternative medicine by 2010 [2]. Asian governments are pouring billions of dollars into screening Traditional Chinese medicines in the hope that clinical trials will spawn lucrative drugs [3]. Traditional medicine has become big business.
Indeed, it has, which is why I always have to try desperately not to laugh out loud whenever advocates of "complementary and alternative medicine" (CAM) claim it's all about the money for big pharma but not for CAM. But I digress:
While scientific studies have validated some traditional remedies, for instance, by confirming the biological activity of plant extracts [4], [5], the use of complementary and traditional medicines remains contentious, and doubts about the efficacy and safety of many treatments remain [1], [6], [7], [8]. Reservations over safety and efficacy underpin controversy over USA and UK universities' attempts to bring alternative medicines into medical school curricula [9]. The active ingredients used in many traditional medicines are potentially toxic, often containing dangerous elements, including heavy metals [5], [10]. Even the use of ineffective non-toxic remedies can be harmful if it delays effective treatment. For instance, fears have been expressed that, in Nigeria, witchcraft and traditional remedies of unknown efficacy are widely employed as treatments for malaria, instead of, or delaying access to, modern medicines of proven effectiveness [11]. In sub-Sarahan Africa there is a concern that the use of traditional remedies for mastitis, a condition often attributed to sorcery, may inadvertently be contributing to the spread of HIV [12].
In 2002 the WHO [1] launched a global plan to make the use of traditional medicine safer by encouraging evidence-based research on the safety, efficacy and quality of traditional practices. Accordingly, traditional medicines are currently undergoing scrutiny to evaluate their effectiveness and monitor adverse events [3], [13]. Such analyses have often failed to confirm the efficacy of traditional remedies: for instance, of nearly 25,000 applications for registration of traditional medicines received by Malaysian authorities, 37.3% were rejected, either on grounds of safety or ineffectiveness [14]. However, there is currently no compelling explanation for the prevalence of low-efficacy treatments.
As I said before, I never found explanations of lack of scientific understanding or confusing correlation with causation entirely satisfactory, although I do make an exception for people like J.B. Handley and many antivaccinationists, who clearly do lack scientific understanding and confuse correlation with causation. Indeed, I definitely think these are major reasons why, for instance, so many parents believe vaccines cause autism or so many people think that reiki works. I just don't think they're enough.
Tanaka et al basically construct a model in which they attempt to estimate the factors that could affect the spread of various treatments throughout the population. One aspect of this model to be kept in mind is that it primarily looks at self-medication, although parents medicating their children, as happens in too much autism quackery, could be included under this category, mainly because it is not the children who decide for themselves whether a treatment is working or not; it is the parents. The general assumptions of the model are summarized in Figure 1 below:
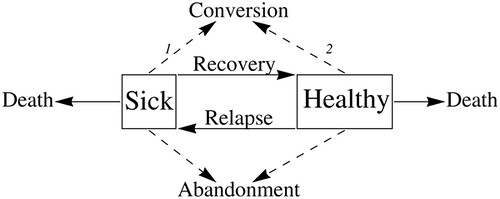
Table 1 lists the parameters inputted into the model:
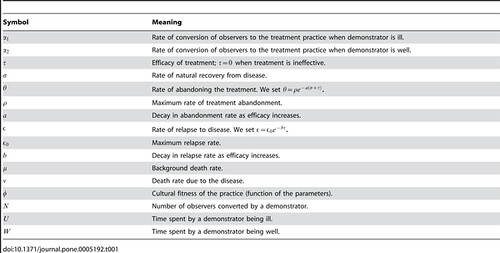
I'm not going to go into the equations in much detail. In fact, I'm not going to go into the equations at all. (Perhaps blogchild Mark Chu-Carroll would be interested in a detailed analysis.) The article is freely available to all; so you can read it yourself. What I will discuss are some of the assumptions going into the model. First among these is this:
We assume that individuals are either in a diseased state or in a healthy state. We model the spread of a behavioural trait expressed in treatment of disease. The behavioural trait in question is any innovation, practice or treatment that could potentially affect the outcome of this disease. To model the spread of a behavioural trait, we make the following assumptions. A new behavioural trait arises in (or is invented by) an ill individual who may then demonstrate this practice; others who are ill may adopt the practice upon being exposed to it, and then become demonstrators themselves. In other words, demonstrators convert observers. There is empirical support for the assumption that self-medicative treatments spread through social learning [22].
The most important assumption made for the model is that observers adopt the trait in an unbiased fashion. The authors don't assume a priori that efficacy has anything to do with whether observers take up a treatment. While this may sound unreasonable on the surface, it is actually a reasonable assumption, as most observers are not very good at judging the efficacy of a treatment. Any regular reader of this blog should be aware of why this is true; it's basically because any observer trying to determine whether or not a treatment is efficacious on the basis of watching it being used on another person or hearing about it, is using either anecdotal evidence or testimonial evidence to come to a conclusion. If there's one theme that's run through this blog from the very beginning, it's how easily we as humans are deceived by anecdotal evidence and that testimonials are usually worthless. Indeed, unless a remedy is rapidly fatal or produces a miraculous recovery, given the effects of regression to the mean, confirmation bias, treatment bias, and a variety of other biases, judging the efficacy of a therapy on the level of an individual can be very problematic even for physicians. For the untrained, it's really probably very close to random chance whether a person judges the efficacy of a treatment correctly. Actually, it's probably even worse. As I have said, we humans are very good at deceiving ourselves.
The authors define the "cultural fitness" of a treatment as the mean number of converts produced by a demonstrator and then studied what the value of cultural fitness would be under various assumptions, both for instances of single illness and in the case of multiple relapses of illness. Interestingly, although highly efficacious treatments are predicted to spread through the population, even in the case of inefficacious treatments, multiple exposures of it and a remedy for it actually increase the chance that the treatment will spread, reagardless of whether the treatment is efficacious or not. The authors concluded that, although highly efficacious treatments have a high cultural fitness, treatments with efficacy near or at zero can also spread. The conditions under which such remedies could spread and achieve high cultural fitness are when treatments are primarily demonstrated in sickness and demonstrate low abandonment, particularly where the likelihood of relapse is small. The authors summarize:
This study offers a simple, novel and counter-intuitive hypothesis for the prevalence of ineffective medical treatments: unbiased copying of new treatments can frequently lead to the prevalence of ineffective practices because such treatments are demonstrated more persistently than efficacious alternatives, even when there is enhanced abandonment of ineffective cures. By unbiased copying, we mean copying in direct proportion to the rate at which the alternative variants are demonstrated. Here, in simple terms, treatment frequency dynamics are typically dominated by two processes, representing the rates of acquisition and loss of remedies. Maladaptive and superstitious treatments can become prevalent because their ineffectiveness prolongs illness, enhancing their rate of demonstration relative to efficacious cures, and leading to elevated rates of acquisition that may compensate for greater loss.
Our finding that superstitious treatments can easily spread is supported by reports of extraordinary treatments for conditions such as leprosy (treated with a drink made of rotting snakes) and syphilis (treated by eating a vulture), and by similar myths for poisonous snake bites (apply 'guaco' leaves, poisonous lizard skin or snake's bile), dog bites (drink tea made from the dog's tail) and scorpion stings (tie a scorpion against the stung finger) [23]. The analysis also helps explain the persistence of medical treatments of animals, such as 'firing' (cautery) of working horses, employed for millennia as treatment for lameness, where recovery is rare, and still widely practiced in many countries in spite of trials establishing its ineffectiveness [24].
Another conclusion of this model is that even highly effective treatments can be lost due to stochasticity, in other words, due to random chance. Indeed, the authors point out that most highly efficacious innovations would be predicted to be lost due to stochasticity. Indeed, my reading of this study would suggest that one reason why highly effective treatments actually do persist in our society is because scientists, physicians, and science-based medicine validate what treatments are efficacious, retaining the treatments that are and trying (but not always succeeding) in discarding the ones that aren't. For people self-medicating, such a mechanism is not operative.
One aspect of this model that I consider inadequate is that it doesn't take into account the role of peer pressure and groupthink. It certainly doesn't take into account the rapidity with which glowing stories of success for quackery can spread through both word of mouth and other methods. In this case, the Internet truly has changed everything. Never before, has it been possible for so many people to "listen to so many stories" in such a short period of time or to form online communities made up of people who mutually reinforce each other's beliefs, even though most of them have never met face-to-face.
I return to one of my favorite examples, autism quackery such as "biomedical interventions" and chelation therapy. Because autism is a condition of developmental delay, not stasis, it's very easy to confuse correlation with causation and believe that a given ineffective intervention "worked." Prometheus points out this very phenomenon:
If you have the opportunity, check in to one of the many "biomedically oriented" Internet groups and see what happens when somebody questions the idea that "biomed" can "recover" autistic children. At the least, they will be admonished - "Don't stand in the way of other parents getting their children the help they need!". More likely, they will be told to "Shut up!" and banned from the group. In some cases, they will be harassed and even threatened.
I'm not sure how the authors could have modeled the "Emperor's New Clothes" phenomenon, such as Prometheus describes, but I can't help but think that such mechanisms are at work in addition to the ones described in this paper. On the other hand, this model strikes me as useful for explaining the antivaccine movement. Vaccines are never "demonstrated" to cure a sick person; rather they prevent people from ever getting a particular disease, which means that this method of spreading in a population according to this model would not drive the use of vaccines. However, seeing rare adverse outcomes, given that the diseases these vaccines prevent are, thanks to the vaccines, no longer common, would lead people to see the outcome of vaccines as more negative than positive even though the evidence is overwhelming how the benefits of vaccines outweigh the risks.
Another aspect of this model is whether it can be modified to account for what I'll call the "Oprah Effect." This effect is due to highly influential (and often credulous) media people promoting a treatment to millions in the population, as Oprah does for various woo like The Secret, Mehmet Oz, or the various other dubious "experts" who are regulars on her show. I would label people like Oprah "super-demonstrators," because through their efforts they can greatly increase the number of "demonstrators" in a population. Such a phenomenon undoubtedly went on to a much lesser extent in traditional societies in the form of shamans, chieftains, and village elders, but with mass media and the Internet the ability of such "super-demonstrators" to pump up the numbers dwarfs what could ever happen in a traditional society living a hunter-gatherer or early agrarian kind of existence. My guess is that it wouldn't be too difficult to ad a factor to the model to account for "super-demonstrators." I would also guess that the existence of these super-demonstrators would make it even more, not less, likely that ineffective or maladaptive treatments would spread through the population. But that's just a guess.
As much as I like this paper for its description of a plausible mechanism by which implausible and ineffective treatments can spread through a population and remain entrenched, I have to caution that, without some sort of experimental or observational validation, it remains just that: a model. Unfortunately, I'm having some difficulty figuring out just how one might test this model against reality in a real human population.
One thing that this model leads me to wonder, though, is whether, maybe--just maybe--there is a force that can prevent or halt the spread of implausible, unscientific, and ineffective treatments, such as homeopathy, throughout the population. Perhaps such a method both serves as a memory that recalls which therapies don't work and a method of testing which methods do work. That method is science- and evidence-based medicine.
I wonder how the effect of physicians supporting SBM and teaching it to their patients can be incorporated into this model. What I fear, given the infiltration of quackademic medicine into academia, is that what we'll really have to add to the model is a factor to account for physicians also reccomending ineffective woo.
This is pretty interesting. Have you ever written on self-help groups like AA; or , if not, do you have any thoughts on the subject (in this context)?
Further to above, I guess what I find so interesting with respect to self-help groups is the novel thought that they are not so much groups that collect "patients" as groups that collect observers. I sense also that there is a lot of food for thought in the dynamics of recovery, relapse, abandonment etc. I will try to read the original article, and get as much out of it as I can.
Not to be direspectful, but I disagree with your conclusion. Evidence based medicine has not yet served as that memory, as all the evidence of increasing woo should be telling you.
It is science based medicine that needs the "super demonstrator". Since Carl Sagan, there has yet to be an effective populaizer of science that speaks in voice that is easily consumed and diseminated. One of the reasons is that too many science based voices insist on describing "why" and "how" in detail and most people don't care. They didn't need a detailed explanation of "why" something works from Chopra, they don't need it from you.
The explanation of "why" and "how" is dehumanizing. The similar dismisssal of the placebo effect is also dehumanizing and the average human is, well, kind of put off by being dehumanized. They tend to cling to that human thing. Go figure.
Modern science has forgotten that in terms of usability and consumability, the "why" and "how" doesn't really matter. Those that eat sausage don't want to know how it is made, they just want to eat something that is tasty and works (this applies if the sausage is made of tofu as well, please don't lose focus on arguments of the eschatology of diet).
That same applies to medicine and science in general. If we follow the evidence, it is obvious that what is more important in the woo/science battle is who appears more human and authoritative. The perceived difference between Depak Chopra and, say, your average doctor on CNN, is that Chopra never appears to have any doubt. He recognizes and emphasizes the human-ness of his reccomentdations and looks the viewer in the eye. Doctors speak in terms of probability and mechnisms.
There is good reason doctors do that (not only moral but litigous forces compel it). But there is also good reaason for the modern medical establishment to recognize that in questions of public health (and health policy), the message is as important as the treatment. The evidence of increasing resistance to effective treatments for infectious diseases is alarming and the methods used to combat that arrogance of ignorance simply isn't working.
WARNING: Jim Carey has just written an article on Huff Post about vaccines. Enjoy!
http://www.huffingtonpost.com/jim-carrey/the-judgment-on-vaccines_b_189…
I have no problems with wooies refusing antibiotics, at least the adult ones. It's like Jehova's Witnesses dying without blood transfusion, you choose your own poison. It's the children's suffering that gets to me.
What makes me wonder, if the ND detects child abuse in the form of untreated infections due to his own "treatment", does he have to report himself or is he protected by the 5th?
Are you on ResearchBlogging.org? You should add the icon to this post.
Coturnix, the icon was used when he posted that article on the other blog with his real name.
Orac is completely correct in saying humans are very good at deceiving ourselves. Just look at hiv/aids theory over the last 25 years.
A kind of collective insanity over HIV and AIDS has gripped leaders of the scientific and medical profession. They have stopped behaving as scientists, and instead are working as propagandists, trying desperately to keep alive a failed theory."
Neville Hodgkinson, former Science Editor, The Times of London
Orac, I think you are on to something when you propose the idea of "super-demonstrators". There *are* differences among demonstrators. It might be useful to turn the microscope around and ask, "why are advocates of SBM failing to be persuasive demonstrators and super-demonstrators?
I am reminded of the placebo studies which show that a blue sugar pill is more effective than a red sugar pill.
When people visit a doctor, he is often running late. Insurance companies don't allocate much time for office visits, so he finds himself playing catchup all day. He is tempted to rush through a visit that seems straight-forward, like an ear infection. Short office visits don't allow time to talk about prevention, or lifestyle choices, or diet, let alone time to banter about "how's life treating you", "how are the kids", "still playing tennis", etc. In addition, many physicians are impatient with questions. I think this is changing, but many are still locked into the idea that patients should simply trust their physicians.
Contrast that with a visit to a woo-meister's office. They can charge for as much or a little time as you have money to pay for. Not only are they interested in all the minutia of your personal life, they tell you that it is all an important part of their holistic approach to treating the "whole person", not just symptoms. What an appealing idea!
(Who *WOULDN'T* want Deepak Chopra as their grandpa? He's a sweetheart! a teddy bear! So wise! So patient! Every word as soothing as chamomile tea!)
I think that SBM has a bad PR problem resulting from problems in the medical *system*. Most people at some point or another feel let down by the healthcare system. It doesn't logically follow that science based medicine is ineffective. But it does leave patients receptive to alternatives, especially alternatives that are tailor-made to appeal to people who have been frustrated by the establishment healhcare systems that provide evidence-based medical care to patients.
I am tempted to let "Neville" know exactly what I think of his brand of delusion (one I once entertained out of ignorance and fear), but unless he's degenerated to referring to himself in the third person, that's most likely not really him and is a shoddy attempt to derail the thread.
But I digress . . .
I read this article (and Terry's post) with great interest, as I was once one of the people science is trying to reach. Reasonably intelligent, well educated and professional but very, very fearful. Fearful of dying, fearful of "cold" doctors and scientists and drawn to the comforting siren song of "heart" and woo. Now, while I wasn't totally credulous, I was willing to suspend my reasoning mind enough to fall for all manner dubious-yet-comforting ideas. I hated skeptics and critics. Maddox, Gardiner and Dawkins (now my heroes) were evilâthey were "snowman melters". They didn't have a heart. They were unimaginative at best and dehumanizing at worst. What I didn't realize was that the reason I disliked them was that I feared them, and I feared them because I knew they were right. I won't go into the long story of my awakening from fear and denialism here, but suffice it to say that the events that started the chain of events that led me to reason were momentous. One thing I do know, is that I always had an innate skepticism simmering underneath the surface, so I've been pondering the question: what, if anything, would have changed my mind at 25 or 35, instead of 45? Without the aforementioned momentous events, would I still be credulous enough to question HIV as the cause of AIDS? Would I still believe that we are more than our brains and that I would outlive my body? I guess I can't really know that, but you all will be the first to know if I figure it out. I wonder if Oprah would feature a book about a journey OUT of woo?
"Dehumanizing?"
Sigh. Yes, by all means, let's abandon rationality in favor of what makes us feel good. Especially when it comes to prolonging our lives. And let's insult those who are doing the work of prolonging our lives for telling us something other than what we want to hear.
I work in government health promotion. The only ethical thing to do in that field is to accurately communicate science-based information. We can--and should--tune the message to make it more clear, and even more palatable. But we can't abandon promoting the scientific basis for health-related decisions. That's abject nonsense.
Landru, if you're referring to my post, the "dehumanizing" quote represented my former belief system, the fear based one that led me to believe a lot of very wrong things. I agree that science needs to pull no punches when it comes to dealing with pseudoscientific misinformation, however, as a communications professional, I'm trying to find ways to get the message across to those who are fearful of science. These folks simply shut down when they feel attacked. Those who know my blog would find that kind of ironic since I'm a total polemic smartass in my approach to magical thinking, but that work is meant to make my fellow skeptics laugh, not convert the magical thinkers. I agree totally that it would be abject nonsense to abandon promoting science for health-related concerns, but it certainly wouldn't hurt to find and groom an appealing, Saganesque spokesperson who could reach through people's fears of the unknown and inspire them to learn. I don't have the answers, but I'm asking the question from the perspective of someone who has made the very change in thinking that we're seeking to promote.
Indeed, I mean hell lets start prescribing sugar pills again! That's ethical! And it works way better, didn't you see that episode of MASH?
Yea! Let's go back to that! Let's go back to when all you needed to trust your doctor was to know they could look you right in the eye and had a damn firm handshake!
Back when charisma and a nice suit were enough to get you lots of patients and sacks full of money, the hell if you don't actually help anyone!
While we're at it, can we bring back leeches?
I'll agree that SBM lacks a good PR rep right now though, I don't have a great solution for that. Except to suggest that Orac go on the TV circuit.
P.S.: My apologies if my post has missed Terry's point, I'm snarky today.
While we're at it, can we bring back leeches?
They're already back, they're a great boon for reducing the complications from crushing injuries.
Is woo actually increasing? or has it simply come out of the woodwork and become more visible.
I would prefer not to have any super-demonstrators in science due to over-reliance on a few people.
Pareidolus, you weren't the one who introduced the notion that explanations are dehumanizing, and you're not the poster who made me feel like I couldn't shut up. In fact, I only partially understood what that word was getting at until I read your comment.
@Snerd
Ya know, I shouldn't have been glib with the leeches comment, I actually have seen leeches used, as well as maggots.
Perhaps I should have been more specific about which uses of leeches should be brought back.
Or perhaps I should have made a tasteless remark about homeopathy and magic potions instead.
Terry suggests that "One of the reasons is that too many science based voices insist on describing "why" and "how" in detail and most people don't care."
There may be people who are naturally like that, but I, and it seems to me a lot of people, have a lot of curiosity. If I do not understand what is going on, or if I do not know how something works I am not happy until I find out. And if an accepted explanation doesn't make sense I attempt to find one that does make sense. My most innately human characteristic is curiosity - being prevented from knowing the "why" and "how" is - for me - extremely dehumanizing.
If faith is supposed to be the answer to the human condition then we all may as well be zombies.
"Sigh. Yes, by all means, let's abandon rationality in favor of what makes us feel good. "
The method and the message are two different things. I am not advocating giving up evidence based medicine, which shoudl be clear. I am advocating the idea that to reach the people that need to be reached, the message and its delivery has to change. Jenny McCarthy has more gravitas than a scientist. Think about that. And then tell me whether or not you think EBM has done an effective job of getting the message out correctly or not.
You can be snarky is you wish, but the problem is real. And it needs to be solved for, because we are all at risk if vaccinations and sound medical practice continue to be attacked in this way.
"But we can't abandon promoting the scientific basis for health-related decisions. That's abject nonsene"
Ignoring evidence is abject nonsense. Promotion is a valid subject. But when it is the entire message it doesn't work. The proof is right in front of your nose if you read this blog as I do. How can you not be distrubed by this ant-vax nonsense?
"There may be people who are naturally like that, but I, and it seems to me a lot of people, have a lot of curiosity"
Are you suggesting that if a true and effective evangelist appeareed on Oprah and got the right message across that orac and all his blog posts would just disappear in a puff of illogic? There will always be sources of information for those that want it. But last time i checked there was a far larger world than the one that read this blog and they aren't going to suddenly abandon woo if you put make them read these posts.
"While we're at it, can we bring back leeches?"
Yes, let's abandon SBM because if an effective communicator appears, that illogic will suddenly bias and pollute all science and medicine. Brilliant.
"P.S.: My apologies if my post has missed Terry's point, I'm snarky today"
Indeed.
"If faith is supposed to be the answer to the human condition then we all may as well be zombies."
Oh, but zombies do exist. That's the whole point of fighting woo and why it is so dangerous. That's why when whole communities abandon vaccination is dangerous to all of us. The question you should be asking is "how do I communicate with a zombie?" You may think that harsh, but I think the job of medicine is to make people better, not make better people (to borrow a phrase).
"Dehumanizing?"
Yes and I stand behind it. It wasn't that long ago that doctors were trusted. I'm old enough to remember what that was like.
I contemplated a substantive response, Terry, but your view that "Jenny McCarthy has more gravitas than a scientist" makes me perfectly happy to allow you the last substantive word on this, and sorry that I tried to engage the likes of you in the first place. Totally my bad.
Are you deliberately trying to misunderstand/misrepresent me? That's not *my* view. I am saying that to the people that watch Oprah/Larry King/etc, Jenny McCarthy has more authority than an educated, informed scientist/doctor. And there are more of those people than there are of us. Burying our collective heads in the sand and pretending that it isn't true is the kind of behavior that I would expect from Age of Autism.
Wow. Low opinion of the proles, then?
Joke. Really. I'll peaceably accept your explanation that your writing style was ironic, despite the appearance to the contrary, your naked and unwarranted hostility toward me, and your raw condescension toward the less educated and less intelligent (who are, as you have in fact implied all along, most in need of tailored health promotion messages that suit their personal listening and comprehension propensities).
Okay, I'm vented now.
I don't mean to trivialize the issue of promoting health to educationally diverse audiences. I disagree completely with your assertion that "there are more of those people than there are of us." To the extent that there are data, they tend to suggest the converse--the proportion of people in wealthier countries who are actually vaccinated, the continuing improvements in trends in mortality and disability attributable to preventable causes--but it's a stretch for me to call those things data. Without real data, we can assert at each other all day and it'll just degenerate, so I'm happy to stipulate that we've now mutually and clearly asserted on that item.
Antivaxxers are noisy and ignorant, and when you rile them up, they make my puny efforts at antagonizing you over your writing style and choice of words like "dehumanizing" look even more puny and irrelevant. Further, it doesn't matter how things are explained to them (or not). Arguments from fact, evidence, and logic are all rejected with force, hostility, and paranoia. In the specific case of antivaxxers, I think all that can be done is to limit the spread of the ignorance. There will, for a very long time, be a hard core that will remain unconvinced, despite all efforts.
Would I blow you off if you suggested a specific alternative messaging strategy with some prospect of success? Nope. But you haven't, and I defy you or anyone to do it. With the antivax hard core, it's no longer about messages or truth. It's about paranoia, fear, blame, and quite probably shame (which is sad and unfortunate). Way easier to just limit the damage and refute the lies.
Those are reasons we shout here as we do, and the same issues complicate the general challenge of communicating any health promotion messages to the public. Oscar Zoalaster (above) is correct in that a nontrivial (maybe significant, maybe even substantial) proportion of people do want explanations. Should docs obtuse a message into oblivion? Of course not. Providers and other communicators should tailor their health promotion messages to the audience--just like any other messages. A variety of approaches is required.
Dumbing down the message too much just makes the message dumb. More often than not, that isn't appropriate for communicators who need to remain credible in the face of (as you acknowledged) a potentially litigious world.
A side note: after JMac's initial appearance on Larry King last year (the one where she shouted down prevention-minded docs and scientists, screaming obscenities), I called my elderly mother, who I knew would have been watching. Now, she's a retired nurse, so it skews the already miniscule sample, but she's also kinda new-agey and crunchy, so I was a little concerned about her perception. She had no trouble at all understanding that JMac was full of it, and that King was more full of it for giving her a platform.
Oh, bugger. I just used an anecdote as data. What an outstanding way to wrap up 15 minutes of brilliant written argument in this forum...