
"Alternative medicine," so-called "complementary and alternative medicine" (CAM), or, as it's become fashionable to call it, "integrative medicine" is a set of medical practices that are far more based on belief than science. As my good bud and collaborator Mark Crislip so pointedly reminded us last week, CAM is far more akin to religion than science-based medicine (SBM). However, as I've discussed more times than I can remember over the years, both here and at my not-so-super-secret-other blog, CAM practitioners and advocates, despite practicing what is in reality mostly pseudoscience-based medicine, crave the imprimatur that science can provide, the respect that science has. That is why, no matter how scientifically implausible the treatment, CAM practitioners try to tart it up with science. I say "tart it up" because they aren't really providing a scientific basis for their favored quackery. In reality, what they are doing is choosing science-y words and using them as explanations without actually demonstrating that these words have anything to do with how their favored CAM works.
A more important fundamental difference between CAM and real medicine is that CAM practices are not rejected based on evidence. Basically, they never go away. Take homeopathy, for example. (Please!) It's the ultimate chameleon. Even 160 years ago, it was obvious from a scientific point of view that homeopathy was nonsense and that diluting something doesn't make it stronger. When it became undeniable that this was the case, through the power of actually knowing Avogadro's number, homeopaths were undeterred. They concocted amazing explanations of how homeopathy "works" by claiming that water has "memory." It supposedly "remembers" the substances with which it's been in contact and transmits that "information" to the patient. No one's ever been able to explain to me why transmitting the "information" from a supposed memory of water is better than the information from the real drug or substance itself, but that's just my old, nasty, dogmatic, reductionist, scientific nature being old, nasty, dogmatic, reductionist, and scientific. Then, of course, there's the term "quantum," which has been so widely abused by Deepak Chopra, his acolytes, and the CAM community in general, while the new CAM buzzword these days to explain why quackery "works" is epigenetics. Basically, as I pointed out earlier this week, whenever a proponent of alternative medicine uses the word "epigenetics" or "quantum" to explain how an alternative medicine treatment "works," what he really means is, "It's magic." This is a near-universal truth, and even the most superficial probing of such justifications will virtually always reveal magical thinking combined with an utter ignorance of the science of quantum mechanics or epigenetics.
So, yes, much of CAM is either very much more like religion than science in that CAM is immune to evidence. True, the scientific "explanations" change, and CAM practices might evolve at the edges based on evidence, but the core principles remain. You don't see, for example, homeopaths or naturopaths deciding that homeopathy doesn't work because science and clinical trials overwhelmingly show that it is nonsense. You don't see chiropractors leaving chiropractic in droves because they've come to the realization that subluxations don't exist and they can't cure allergies, heart disease, gastrointestinal ailments (or anything else) but rather are in reality physical therapists with delusions of grandeur. Ditto reiki, acupuncture, therapeutic touch, and "energy healing." These practices persist despite overwhelming evidence that they do not work and are based on magical thinking, not science. All of the scientific studies and clinical trials funded by NCCAM and other CAM-friendly organizations never actually take the next step from all the negative studies of CAM and come to the conclusion that they should stop using such modalities.
No one is saying that the record of SBM is perfect when it comes to changing nimbly with new evidence, and any imperfection in the record of SBM and evidence-based medicine (EBM) actually being, well, science- and evidence-based, is a favorite target of CAM apologists. Hence there are frequent claims circulating that only 15% of medicine is actually evidence-based. It's a bogus claim, a myth, as Steve Novella has pointed out. In reality, studies appear to converge on estimates that approximately 80% of interventions are based on compelling evidence, and between 30-60%, depending on the specialty, are based on randomized clinical trials. That's not good enough, but it's far better than CAM apologists would lead you to believe, and it's certainly far better than anything in CAM.
Nonetheless, it has been recognized for a long time that EBM/SBM is sometimes slow to change in response to new evidence. Indeed, there was an aphorism I heard while in medical school that outdated treatments and procedures don't die off completely until the physicians who learned them during residencies or fellowships die off. I learned that that's not entirely true. There is, after all, a gap of around 20 years between the time a generation of physicians retires and dies off; so such practices actually die off much sooner. I keed, I keed, of course, but the point is valid.
There is the opposite problem in EBM/SBM as well, namely a tendency towards a "bandwagon" effect wherein a new therapy is widely adopted before there is solid evidence of its superiority (or at least of its non-inferiority with alternate benefits). I'm a surgeon, so I know that, unfortunately, the surgical world is very much prone to this sort of problem. Surgeons tend to like shiny, pretty new toys and to do spiffy new procedures that prove that they are the biggest, baddest scalpel cowboys in the all the land. These tendencies have led to a number of procedures becoming widely adopted before they were definitely shown to be superior. Laparoscopic cholecystectomy is the example that I like to use the most; it swept the surgical world over 20 years ago without compelling evidence for its safety. Later, it was found that the incidence of common bile duct injury was much higher after laparoscopic cholecystectomy than conventional cholecystectomy. That incidence fell as more surgeons became more facile at the procedure, but it was years before there was compelling evidence that the laparoscopic approach was truly superior. History seems to be repeating itself today with robotic surgery. At the risk of offending some of my surgical colleagues, I've yet to see compelling evidence that doing, for example, a radical prostatectomy with the da Vinci robot is truly superior to doing it using what was the new way ten or fifteen years ago but is now the old way, using laparoscopy. From my perspective evaluating existing evidence, the da Vinci is as safe and effective as laparoscopy, but if it is sufficiently more so to justify its much greater cost I haven't seen the evidence yet. I sometimes joke that if it were possible to do breast surgery (my specialty) with the da Vinci, then I'd be all for it. Maybe I'll have to look into that. I could be bigger than Armando Guiliano, and time's wasting. I probably only have 15 or 20 years left in my career to make an international name for myself.
Yeah, that's the ticket. I think I'll sign myself up for a course in using the da Vinci robot and then figure out how to use it for breast surgery. I'm sure it'll be a hit. So what if a lumpectomy and sentinel lymph node biopsy takes six hours instead of less than an hour and a half to do?
That is sarcasm, in case anyone's thinking I'm serious.
But how often are medical practices found to be ineffective and abandoned? How much do we test existing practices in light of new data? There have been a number of studies looking at this issue, which is already a marked contrast to CAM, where ineffective practices are, as far as I can tell, never abandoned. The most recent of these caught my eye last week. Published in the Mayo Clinic Proceedings by a team from the National Cancer Institute, the University of Chicago (one of my alma maters!), Northwestern University, George Washington University, and Lankenau Medical Center and entitled A Decade of Reversal: An Analysis of 146 Contradicted Medical Practices, this study seeks to get a handle on the answer to that very question for these reasons:
We expect that new medical practices gain popularity over older standards of care on the basis of robust evidence indicating clinical superiority or noninferiority with alternative benefits (eg, easier administration and fewer adverse effects). The history of medicine, however, reveals numerous exceptions to this rule. Stenting for stable coronary artery disease was a multibillion dollar a year industry when it was found to be no better than medical management for most patients with stable coronary artery disease.1 Hormone therapy for postmenopausal women intended to improve cardiovascular outcomes was found to be worse than no intervention,2 and the routine use of the pulmonary artery catheter in patients in shock was found to be inferior to less invasive management strategies.3 Previously, we have called this phenomenon (when a medical practice is found to be inferior to some lesser or prior standard of care) a medical reversal.4, 5, 6 Medical reversals occur when new studies—better powered, controlled, or designed than their predecessors—contradict current practice.4 In a prior investigation of 1 year of publications in a high-impact journal, we found that of 35 studies testing standard of care, 16 (46%) constituted medical reversals.4 Another review of 45 highly cited studies that claimed some therapeutic benefit found that 7 (16%) were contradicted by subsequent research.7
Identifying medical practices that do not work is necessary. The continued use of such practices wastes resources, jeopardizes patient health, and undermines trust in medicine. Interest in this topic has grown in recent years. The American Board of Internal Medicine launched the Choosing Wisely campaign,8 a call on professional societies to identify the top 5 diagnostic or therapeutic practices in their field that should not be offered.9 In England, the National Institute for Health and Clinical Excellence has tried to “disinvest” from low-value practices, identifying more than 800 such practices in the past decade.10 Other researchers have found that scanning a range of existing health care databases can easily generate more than 150 low-value practices.11 Medical journals have specifically focused on instances in which more health care is not necessarily better. The Archives of Internal Medicine created a new feature series in 2010 entitled “Less is More.”12
One can't help but note right from the introduction of this paper that SBM/EBM does continually reevaluate its practices and treatments, testing which ones work and which ones do not and comparing current practice against new treatments. Granted, the intensity of this effort seems to be a more recent development, with the implementation of the Patient Protection and Affordable Care Act, but is it really? This article suggests that the answer is: perhaps not.
The authors specifically examine the question of how much of the medical literature consists of what they refer to as "medical reversals," as described above. Specifically, they tried to estimate what percentage of the medical literature consists of articles that question current medical practice, particularly that consist of high quality evidence suggesting that current practice needs to be changed or that a standard-of-care intervention doesn't work, doesn't work as well as a non-standard-of-care intervention, or is actually harmful. How the authors did this, I find easier to let them describe:
Two reviewers (C.T., A.V., M.C., J.R., S.Q., S.J.C., D.B., V.G., or S.S.) and V.P. read articles addressing a medical practice in full. On the basis of the abstract, introduction, and discussion, articles were classified as to whether the practice in question was new or existing. Methods were classified as one of the following: randomized controlled trial, prospective controlled (but nonrandomized) intervention study, observational study (prospective or retrospective), case-control study, or other methods. End points for articles were classified into those that reached positive conclusions and those that found negative or no difference in end points. Lastly, articles were given 1 of 4 designations. Replacement was defined as a new practice surpassing an older standard of care. Back to the drawing board was defined as a new practice failing to surpass an older standard. Reversal was designated when a current medical practice was found to be inferior to a lesser or prior standard. Reaffirmation was defined as an existing medical practice being found to be superior to a lesser or prior standard. Finally, articles in which no firm conclusion could be reached were termed inconclusive. The designation of an article was also performed in duplicate. When there were differences in opinion between the 2 reviewers, adjudication first involved discussion between the 2 readers to see whether agreement could be reached. If disagreement persisted, a third reviewer (A.C.) adjudicated the discrepancy. Less than 3% of articles required discussion, and less than 1% required adjudication. A table detailing each medical reversal was constructed (Supplemental Appendix; available online at http://www.mayoclinicproceedings.com), and the third reviewer (A.C.) reviewed all reversals.
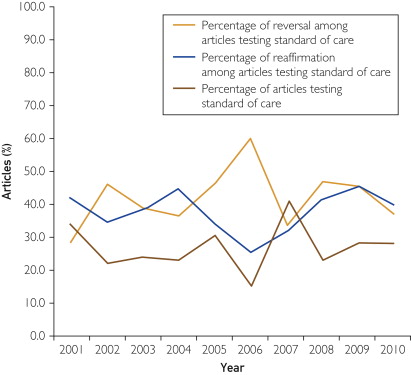
So what did the investigators (Prasad et al) find? They examined ten years' worth of NEJM original reports, from 2001 through 2010, for a total of 2,044 original articles. Of these, 1,344 (65.8%) addressed a medical practice, of which 911 (68%) were randomized controlled trials, 220 (16%) were prospective controlled but non-randomized studies, 117 (9%) were observational studies, 43 (3%) were case-control studies, and 53 (4%) used other methods. Of these 1,344 reports, 981 (73%) studied a new medical practice, while 363 (27%) addressed an existing practice. Overall, 756 articles (56%) found that a new practice surpassed the existing standard of care at the time (replacement), while 165 (12%) failed to find that a new practice was better than existing practices. In terms of what we're really interested in, of the 363 studies examining an existing practice, 146 studies (40%) were reversals, while 138 (38%) upheld standard practices. Here's a breakdown from the article for your edification:

Of the reversal articles, not surprisingly most (76%) turned out to be randomized clinical trials, and interestingly, the percentage of each type of trial didn't change much over the decade-long study period:
The one problem I had with this study was that it only looked at one journal: The New England Journal of Medicine. I can understand why the authors might have chosen that particular journal. It's very high impact, and, with the exception of a recent distressing tendency to let some low quality CAM articles slip in, one of the more rigorous medical journals out there that isn't a specialty journal; i.e., it accepts articles covering all areas of medicine. It's not a basic science journal; it generally only publishes original studies that are either clinical trials, epidemiological studies, or at the very least highly translational. It also, from my reading, only rarely publishes really preliminary clinical work, such as phase I clinical trials. On the other hand, one has to wonder whether the results would be generalizable to the rest of the medical literature.
For example, according to this study, articles in the NEJM that tested new practices were far more likely to find them beneficial than articles that tested existing ones (77.1% vs 38.0%), while articles that tested existing standard-of-care practices were far more likely to find those practices ineffective than articles testing new practices (40.2% vs 17.0%). Looking at such numbers, I can't help but wonder if there is a publication bias for finding new therapies effective and/or for finding existing therapies either ineffective or harmful, particularly in the NEJM, which is among the highest of high-impact medical journals. Think about it. Who thinks that their findings are substantial enough and interesting enough to be seriously considered for publication in the NEJM? It's investigators who have found that some new therapy works for a common or very serious disease, but it wouldn't surprise me if it's also authors who have found compelling evidence that a commonly used existing standard of care is either not effective or is even dangerous.
It's also informative to look at some of the medical practices that were the subject of reversal articles. For instance, it was thought that certain vaccinations could increase the risk of relapse in multiple sclerosis, but two studies showed no increased risk. One looked at tetanus, hepatitis B, and influenza vaccination; the other at hepatitis B vaccination. One showed that delayed drainage of effusion in otitis media did not result in worse outcomes than immediate placement, resulting in a change in practice. Another key reversal came in the form of a 2003 study that showed that high-dose chemotherapy followed by bone marrow transplantation did not improve survival in advanced breast cancer. This was a huge one, and almost immediately oncologists stopped doing bone marrow transplants for breast cancer. Another showed that the use of pulmonary artery catheters in acute lung injury didn't improve outcomes and was associated with more complications. (When I was a resident in the 1990s, all of these patients got pulmonary artery catheters.) A couple of these I've written about, such as vertebroplasty. More recently, there was a study that showed no benefit to routine PSA screening for prostate cancer in American men.
Indeed, I can't help but mention here that the whole reevaluation of routine screening for cancer, such as PSA screening for prostate cancer and mammography for breast cancer, topics I've written about numerous times for this blog, are examples of exactly that: SBM/EBM evaluating current practices in light of new data and determining whether they should be changed or abandoned. Routine PSA screening for men at average risk of prostate cancer has more or less been abandoned, for example, while current mammography practices are being questioned as promoting too much overdiagnosis and likely will evolve in response.
Perhaps the most prominent example of the efforts EBM/SBM makes to continually reevaluate its practices is the Choosing Wisely initiative. Scott Gavura brought it up last year, and I've discussed it in depth myself. It's an amazing effort, in which major medical societies have made a concerted effort to identify the top five "low value" tests members of their specialties routinely use and then try to get doctors to stop doing them. You will never—never—see CAM doing such a thing, mainly because the CAM practices that have value are in reality "rebranded" SBM, such as nutrition and exercise, and the practices that are really "alternative" are virtually universally "low value." Actually, they're of no value, most being based on long-disproven prescientific notions of disease.
One reason why EBM/SBM is slower than we might like to eliminate outdated and ineffective practices is simple. It's not easy. Evidence from science, epidemiology, and clinical trials takes a long time to come in. It's often very messy. When a practice comes into question, there will often be conflicting evidence, and it often takes a number of studies before conclusions about the practice firm up to the point where they are incorporated into evidence-based guidelines and become standard of care.
Often, practices that are later reversed come into usage based on premature and inadequate evidence. Often, small trials look promising, and physicians start using a treatment based on them. Sometimes such practices become standard based on short term outcome measures, and when long term data become available previously unsuspected harms become apparent. Sometimes it's excessive confidence in the appropriateness of the proposed mechanism used to explain why the treatment should work. What is needed, according to Prasad et al (and I agree), is more rigor:
As such, we favor policies that minimize reversal. Nearly all such measures involve raising the bar for the approval of new therapies6, 83, 84 and asking for evidence before the widespread adoption of novel techniques. In all but the rarest cases,82 large, robust, pragmatic randomized trials measuring hard end points (with sham controls for studies of subjective end points) should be required before approval or acceptance. Our position is in contrast to efforts to lower standards for device and drug approval,85 which further erodes the value of the regulatory process.
One can't help but note that this is in marked contrast to CAM studies, in which CAM advocates ask us to accept much less rigorous types of evidence to accept modalities. As Steve Novella has frequently pointed out, as rigorous randomized clinical trials show that most CAM interventions are no better than placebo, the refrain we frequently hear is that we should look at "pragmatic" trials. In this context, pragmatic doesn't mean the same thing. What Prasad et al are referring to are randomized trials that reflect real-world practices. What I mean by "pragmatic" trials in the context of acupuncture are more observational trials of how the treatment is used in the real world. As I've said many times, this is putting the cart before the horse. Normally pragmatic trials are done for treatments that have already been shown to be efficacious in randomized clinical trials. They can't show efficacy by themselves. They are designed to test how treatments already shown to be efficacious in randomized trials function once let "out into the wild" (i.e., the real world). Frequently, outside the rarified, rigorous world of randomized clinical trials, treatments are less effective.
It should also be pointed out that, just because a treatment was "reversed" in a clinical trial doesn't necessarily mean that the older practices reversed were wrong. However, as Prasad et al put it:
The reversals we have identified by no means represent the final word for any of these practices. Simply because newer, larger, better controlled or designed studies contradict standard of care does not necessarily mean that older practices are wrong and new ones are right. On average, however, better designed, controlled, and powered studies reach more valid conclusions.94 Nevertheless, the reversals we have identified at the very least call these practices into question. Some practices ought to be abandoned, whereas others warrant retesting in more powerful investigations. One of the greatest virtues of medical research is our continual quest to reassess it.
So, yes, "conventional" medicine doesn't always get it right. Occasionally it gets it wrong, on rare occasions spectacularly wrong. But unlike most CAM modalities, EBM/SBM is self-correcting. It actually does abandon treatments that don't work. The process might be messy and ugly at times, but it does happen. For example, many years ago, angina pectoris was sometimes treated with a surgical procedure known as mammary artery ligation. The idea was that tying off these arteries would divert more blood to the heart. The operation became popular on the basis of relatively small, uncontrolled case series. Then, two randomized, sham surgery-controlled clinical trials were published in 1959 and 1960. Both of these trials showed no difference between bilateral internal mammary artery ligation and sham surgery. Very rapidly, surgeons stopped doing this operation. A similar example is one I mentioned above: bone marrow transplantation for advanced breast cancer, which was similarly rapidly abandoned after randomized clinical trials showing it to be no better than the previous standard of care. I'm not saying that this happened without conflict or disagreement; proponents of these therapies can always find reasons to discount the clinical trial evidence. But in the end evidence and science do eventually win out.
Now compare this to CAM practices. Can anyone name a CAM treatment that was abandoned by CAM practitioners as a result of research and randomized clinical trials showing that it doesn't work? A single one? I can't, but I don't claim comprehensive knowledge; so if anyone can answer my question, please do.
In the meantime the abandonment of therapies based on science and evidence showing they don't work or that they work far less effectively than previously thought is the key difference between CAM and EBM/SBM. The day that I see a CAM practice go extinct, like bilateral internal mammary artery ligation for angina pectoris, is the day that I might start to take CAM practitioner claims that they are science-based seriously. I doubt that I will see such a thing happen in my lifetime. I doubt it will happen in the lifetime of the current generation of medical students. In fact, I doubt that it will ever happen, because CAM is based far more on belief than science.
"Surgeons tend to like shiny, pretty new toys and to do spiffy new procedures that prove that they are the biggest, baddest scalpel cowboys in the all the land."
You are a doubter and a skeptic. Did you know that these negative thoughts can now be removed with a simple outpatient procedure - the da Vinci robot-assisted lobotomy?
Man, they've jumped on robotic-assisted surgery big-time at the main hospital I practice at. Maybe it doesn't always have better outcomes than traditional surgery, but it sure does cost more.
DB
Toys cost a lot but makes for tremendous advertising.
Paraphrasing: We have the latest shiny new toys. Come help us pay for them!
Can anyone name a CAM treatment that was abandoned by CAM practitioners as a result of research and randomized clinical trials showing that it doesn’t work?
Of course not. Random clinical trials do not work for CAM due to the highly individualized modalities of CAM. Allopathic doctors have been trying to fight CAM using RTCs for years, but once you start looking at case reports and selective case series you can see the clear superiority of CAM.
Another good example is proton beam therapy - it's increasingly being used in the US for prostate cancer with pretty much bugger-all evidence for better outcomes than standard RT. And for patient groups where there might be a genuine benefit (paed and adult brain tumours) there aren't enough patients being treated to get decent trial numbers.
Also always worth remembering the line about "plane crashes happen, it still doesn't mean that magic flying carpets work" whenever you talk about CAM. So often I see arguments along the lines of "Well, conventional medicine has X, Y, Z wrong, so our way is automatically better". err no. It means that medicine is hard.
At one time, people were given electrical shocks. I'm not talking about electroconvulsive therapy; I mean shocked to stimulate muscles. It was depicted on the film version of "The Secret Garden" where the young son of Mary's guardian received shocks. That form of alternative therapy no longer exists. The other one I can think of is "Mesmerism", Franz Mesmer's treatment regime based on "animal magnetism".
Another one is radionics.
Although woo always keeps an arsenal of ancient lore on hand for resurrection, trends come and go:
at one point, Candida ( not the play) was all the rage, now it seems to have died off like unfed yeast.
Nearly each year recently, a new and exotic berry or fruit was discovered and
advertised to be the answer to humanity's ills- acai, goji etc.
Diverse nutrients are supported with so-called NEW, ground-breaking research as well. The woo of today may be the same as the woo of yesteryear BUT the ingredients change ever so slightly- which probably has something to do with the promotion of new products.
So acupuncture will stick around but it will be delivered in sharper new ways. Energy dis-eases will remain a plague but will be diagnosed with new, useless instruments named after more recent actual scientific discoveries: soon even 'quantum' will sound retro.
A good way to check this is to survey alt med reference books from the past:
I have a 1960s compilation of articles from 'Prevention' and a 1990s masterwork put together by an ND.
But Orac wanted "therapies" that went extinct "based on science and evidence showing they don’t work or that they work far less effectively than previously thought", not because they fell out of fashion like pet rocks.
Radionics is still around and still being used. So are orgone generators:
http://www.radionics.org
@ LW:
No, I was agreeing with him ( who am I NOT to?) -
it's merely the superfiicial aspects/ ingredients that go in and out of fashion-
the basic principles remain:
restoring nature, balancing, harmonising, increasing energy or xi, cleansing/ removing toxins,supporting the body so it heals itself, decreasing stress, addressing the spirit et al.
As for Mesmerism/animal magnetism, I'd say it's still around too, just that it's evolved.
I do find this area of medicine fascinating. Medicine is bound to make mistakes, not least because it is impractical to perform clinical trials sensitive enough to detect the sort of efficacy and safety that may only show up once they have been adopted into clinical practice. In some cases a clinical trial is impractical anyway. If medicine never made mistakes we would never see medical progress.
I have been annoyed at times to see those clinical trials cited as evidence that placebos can improve angina, whereas what they proved was that the then current treatment was useless. There are sham knee surgery trials that show the same lack of functional improvement as knee joint debridement that are similarly cited as proof that placebos "work".
By the way, I'm sure I remember a hematologist friend of mine telling me, 10 or more years ago, that fresh frozen plasma used to be used in some condition (burns?) but then it was found that it increased mortality and was abandoned. I've lost touch with my friend, can't find anything about this on-line and have started to wonder if I imagined it. Anyone know?
As for CAM abandoning any practices, the only thing I can think of is the herbal medical treatment Aristolochia, which causes renal failure and cancer, but there are still websites promoting its use, so I don't think that really counts. In any case it isn't inefficacy that has led to its disgrace, but very serious side effects, that no one noticed during thousands of years of traditional use; it was good old epidemiology that uncovered them.
There are plenty of other CAM interventions that should be abandoned for safety reasons, such as chiropractic neck manipulation, but apparently haven't.
CAM is evergreen because wisdom grows wiser the more ancient it becomes. CAMsters love vagueness and mystery, it allows for handwaving and poetry to suffice when marks patients ask for answers. No annoying, actionable facts are necessary, thus facilitating a good night's sleep . . . for the CAMster.
HTMLfail. Cross out "marks."
@ Krebiozen:
And as I pointed out yesterday, some are STILL talking about MMS for malaria, hiv/aids, ASDs.
Would/should any article on CAM modalities be complete without a visit to Joe's new products? How about "Power Plate" to vibrate your flab away? (Special offer for the super deluxe vibrating "Power Plate" with *accessories at $10,000)
http://powerplate.mercola.com/
* comments about the vibrating machine's "accessories" should be carefully worded.
Quack medicines based on radium salts and water crocks like the Revigator for adding radium daughter products to drinking water were popular 100 years ago but are completely unused today. They weren't driven out of practice by RCT though -- it was a spectacularly gruesome death from Radiathor that was widely publicized which began the decline of this form of pseudomedicine. The examples of deaths from radiation from Hiroshima and Nagasaki finally rung down the curtain on this brand of quackery.
A related pseudotherapy still exist. People spend time in mines breathing the radon-enriched air for alleged health benefits. There is a possibility of benefit, called radiation-induced hormesis. It up-regulates expression of the DNA repair enzymes. However, in the absence of an RCT-proven treatment protocol, this seems like a real crapshoot.
Hey Orac, I was perusing Mercola.com (not for the articles, I needed a laugh so I looked at the comments) and found this gem. Have you ever come across a particular form quackery before called "South-Spinning your water"? Here is a link to the blog where I found it...http://2012forum.com/forum/viewtopic.php?f=16&t=20114
People (well, Germans) used to use thorium toothpaste to "radiate cavities away". (I can't seem to find the ad I once saw that said that.)
As for mesmerism, I just heard a radio commercial for a mesmeric weight-loss clinic. They called it "hypnotism", but it's the same thing. (And equally fact-based.)
Can anyone name a CAM treatment that was abandoned by CAM practitioners as a result of research and randomized clinical trials showing that it doesn’t work?
Mercola backed off of high dose vitamin A some years ago because of the conventional test data for smokers, people with oxidative injuries or liver damage.
High dose nutrition from the 40s-50s that became CAM simply has been starved for funds, basically exiled since the 50s from pharma. Well constructed tests that clearly demonstrate known benefits have been stymied for decades. Many of the few tests run involve known contraindications, defective substitutes, or simply miss minimal success conditions by orders of magnitude.
Just because Mercola decided to reject a treatment doesn't mean it became extinct based on good quality evidence. Besides, I've seen megavitamin A therapy still around, usually in combination with other megavitamin therapy. One quack rejecting a treatment doesn't make it extinct.
Overuse of antibiotics for clearly non-bacterial infections by other healthcare providers (read: urgent cares) is one the things that drives me nuts.
I asked a very similar question in a room full of alternative medicine advocates/practitioners ("Has there ever been an alt med therapy/remedy which was abandoned because you discovered it didn't work?") and one person suggested "phrenology."
Maybe. Or, it might be possible to say that phrenologists were a minority of the scientific mainstream of the time and that is why it was thrown out (though that does seem a bit like question begging.) It was clear though that for the vast majority once promoted always promoted.
I found what happened next interesting. After a brief nod to what could be considered "pragmatic trials" ('everyone has to try and see what works for them") there was a full-scale rush to extreme relativism (and idealistic monism.)
"Reality is whatever we think it is. There is nothing outside of Consciousness. Therefore, ALL remedies work ... but only if you believe in them. No right, no wrong -- just different. The entire scientific paradigm is misguided because it ignores the spiritual nature of reality and the fact that we are all on different levels of awareness." (paraphrased)
Mind you, they are always quick to cite any science-y study which seems to support alt med. At least, they used to before they realized I was probably going to look them up later.
Saying that a medicine is "alternative" is just like marking a belief as "faith." It's an immunizing strategy which tries to have its cake and eat it too.. When the evidence seems to point their way they crow in triumph over how closed-minded the skeptic/atheist is. "Reasonable faith."
But when they are forced to admit the strong evidence is lacking then belief becomes a test of character, of heart as opposed to head. . "No, not all reasonable people will be convinced -- but all the good ones will."
At least SBM doctors usually listen to EBM recommendations.
Quacks would never list to other quacks unless they realize they can make more money off of their victims by doing so.
This might be slightly OT, but something curious happened yesterday and I'm trying to think what, if anything, it reveals about the CAM mindset. Or mine.
In brief: a friend who is a staunch altie finally decided to go to an actual doctor -- a spine specialist -- when her partially paralyzed hand/arm wasn't improving despite the extensive program of quackery she had undergone (for Lyme disease; toxins; etc.) She had originally been told (by 'doctors') when her finger went numb that she probably had a pinched nerve and needed an MRI to find out -- which she refused to do. So she was afraid this was what it was.
Turned out she loved the spine specialist. He told her that he didn't think it was a pinched nerve -- it was arthritis. And she needed no MRI. He and one of his colleagues would treat the arthritis just fine.
But here's the odd part: he explained to her that he could refer her to a neurologist or neurosurgeon and "they will probably tell you something else." Then she would have 2 different diagnoses and she would be "confused" and "conflicted." Being conflicted was so, so hard. You don't know who to believe or what to do. So ... it was totally up to her. If she insisted then he'd refer her to another doctor who would probably want an MRI OR she could just trust that he knew what he was doing, which he did.
Now it gets stranger: my friend told this story as a wonderful example of a medical doctor who had genuine humility. She couldn't believe how humble that was! He could have been arrogant and urged her to get a second opinion .... but he recognized the danger of 'conflict.' He didn't want her to worry. She loved his compassion and sensitivity and ... humility.
WTF?
I have a bunch of problems with this (not least being his apparent assurance that a neurologist would almost certainly tell her it wasn't arthritis) -- but most puzzling I think is that this was categorized as "humility." It sounds like the opposite to me.
I'm interested to get some SBM reactions. Am I missing something obvious ... or do alties really translate 'paternalism' into 'respect?'
(Btw, it's also possible that this "real doctor that (Sastra) would approve of" wasn't anything of the sort: she really can't tell what is and what isn't scientifically accepted. )
Mark Thorson,
Nope, still in use.
Devices that put out enough electricity to cause electrical burns are also still in use.
Evidence that "Terminator Zappers" can cause electrical burns.
@ Sastra
I can't get over that recommending a second opinion is arrogant. How bizarre! The many times I've recommended a second opinion, I've been thanked because it was interpreted that I was doing the best thing for my patient (admittedly, a pet, but still my patient.) I don't recall EVER losing a client over recommending a second opinion. (I did FIRE a few clients over the years, but that's a totally different thing.) :)
@ Sastra:
Perhaps she liked him because he told her what she wanted to hear:
"This is not a big deal and you don't really don't need those new fangled tests. Trust me".
Although he WAS patronising," Don't you worry about it" and he 'protected' her from having to decide ( two diagnoses), his attitude of self-assured certainty and concerned 'care' might have seemed familar to her- like her altie providers.
I read and listen to alt med mavens who seem- to me- to be patronising because they not only know better than the patient BUT they know better than EVERYONE. And they let everyone know.
They have no respect for opinions other than of those who agree with them.
@ Krebiozen @ # 29...link fail
I don't imagine you mean this bug zapper, do you? (Works on one AA battery on mosquitoes and the no-see-ums on my back deck)
http://www.walmart.com/ip/BiteShield-Electronic-Racket-Zapper/11988154
@janet and Denice:
Thanks for the reality check. I figured she would like being told what she wanted to hear ... it was just the insistence that something extraordinarily 'humble' and unexpected from a standard physician was going on which puzzled me.
As I think more about it, I'm starting to suspect that the specialist's admission that "every doctor is going to tell you something different" may be the thing which tripped her admiration. As I wrote above, my altie friends are enamored by the idea that all treatments are fine and will work as long as you believe in them. Nobody is ever wrong; there are no standards to measure by but whatever 'works' for the individual. If there is conflict, then someone is coming from Ego. Avoid conflict.
Whether he intended it or not, it sounds like the spine doctor fed into the fantasy of raging relativism. Which then translates into "humility" (reason = ego, per Course in Miracles.
Sastra - is it possible the spine specialist wasn't a chiropractor? Just asking.
The woomeisters seem to be in a pet about vaccines and "toxins" and "modern life" in general causing a dramatic upsurge in autoimmune diseases, so how do they explain that far and away the most common autoimmune disease—(rheumatoid) arthritis—doesn't seem to be participating in this explosion? You'd think you'd see it there first.
OT, I guess, but Sastra mentioning arthritis made me think of it.
@ Sastra:
"all treatments are fine and will work as long as you believe in them"...
Right. I suppose because then their spirits are "set free" allowing their bodies to "heal themselves".
Seriously, I could get a job writing copy in woo-ville.
Fortunately, I have money.
One practice that was once considered the apex of scientific medicine has been shown to be useless nonsense but still retains it's loyalists: Freudian psychotherapy, which is predicated on the idea that we all have a subconscious as subtle and witty as a 19th Century Viennese physician.
As Lilith put is so nicely in an episode of "Cheers", ",,,his theories are outdated sexist superstitions unsupported by a shred of clinical evidence." And when Frasier suggests using hypnotism on someone, she says, "Hypnosis, Frasier? Why only go back a century for your treatment? Why not bleed him with leeches, or drill a hole in his cranium and let the evil spirits leak out?" Come to think of it, is anyone still using trepanation for anything anymore?
Quick update: the link finally opened and apparently someone does.
http://www.trepanationguide.com/index.htm
lilady,
That's odd, that link worked earlier. Anyway, it's a gadget based on Hulda Clark's zapper, but super-powered and equipped with an orgone generator, crystals, and a mobius coil, all of which are supposed to kill all the parasites we are all supposedly infested with, but which in fact inflicts nasty electrical burns - I have seen photos. Dangerous woo of a high order, in other words.
That link does work, it's just veeeeery slooow, The video of burns caused by this gadget, should anyone care, is here.
orgone generators ....really :?
Well we attach this to your head then turn it on and you are orgone
Delurked Lurker,
Really. I don't know why I find these bizarre gadgets fascinating. Some people enjoy watching sports, I enjoy observing weird beliefs...
Orgone accumulators 'work' by trapping orgone in a box constructed with walls made with alternating organic and inorganic materials, such as steel wool and plastic sheeting, though how orgone knows only to travel one way and not the other through these layers beats me. Orgone generators are constructed by embedding bits of metal (offcuts from lathes are recommended) in resin, along with some crystals and coils. I don't pretend to understand how these are supposed to work, since they don't appear to even pretend to follow any logic whatsoever.
I think I've mentioned here before Don and Carol Croft's adventures tracking down the fiendish Illuminati through Carol's psychic powers, and then foiling them by planting orgone generators near the Illuminati's places of operation. There's a whole world of madness to be explored, should you have the stomach for it! They also have a large section on whale.to, not surprisingly.
Mephistopheles O'Brien #34 wrote:
Yes-- meaning he wasn't. He told her she could go back to her chiropractor who -- in an unexpected burst of ethics -- had been refusing to treat her in case she had a pinched nerve. I really hope she doesn't.
Sastra - Thanks. I know I wrote that badly, but you know when someone talks about a spine specialist that doesn't like second opinions, I get curious. That and I need new computer glasses.
To quote Steve Martin, as a good way to end a Friday when one is feeling completely fried:
It's so hard to believe in anything anymore. I mean, it's like, religion, you really can't take it seriously, because it seems so mythological, it seems so arbitrary...but, on the other hand, science is just pure empiricism, and by virtue of its method, it excludes metaphysics. I guess I wouldn't believe in anything any more if it weren't for my lucky astrology mood watch.
--Comedy album "A Wild and Crazy Guy"
The outrageous fakes and some unwashed fools drooling over sacred cow poop, is exploitation of low entertainment and guilt by association.
A more important issue is about those facts and techniques that have been exiled to the CAM tent, perhaps with Nifong quality "proofs", are being resisted from being mainstreamed or well evaluated at some level, and are further dismissed by "guilt by association".
Kind of reminds me of rumors or accusations that some skeptics are pedophiles being used to sully all skeptics.
prn,
Citations for these “Nifong quality “proofs”” please.
If, as I suspect, you are referring to Moertel’s Mayo Clinic ascorbate trials, perhaps you might comment on clinical trials NCT00441207 and NCT00626444 which used IV ascorbate at the CAM-recommended levels, were completed 2 or 3 years ago, but the results of which remain unpublished.
You continually mutter darkly, implying deliberate dishonesty intended to suppress the truth about ascorbate’s effects. Special pleading about ascorbate having to be combined with whatever, or IV ascorbate only being effective in certain cases doesn't cut it, especially since Cameron and Pauling claimed spectacular cancer cures across the board with ascorbate only. Here's what Cameron wrote:
Wouldn't results like this be easy to replicate?
No one is stopping you from making a case for any of these exiled “facts and techniques”, backed by plausible mechanisms and at least some evidence (by which I don’t mean n=1 self-experimentation). You, or CAM practitioners using these techniques, could even submit case studies to NCCAM or OCCAM which have best case series criteria for CAM practitioners to follow.
If you don’t have compelling case studies to support these “facts and techniques”, what reason do you have to believe they are true/effective?
As for your comments about skeptics and pedophiles, as is very often the case I’m not clear what you are implying. You have a habit of writing in a curiously over-erudite manner, as if convoluted language might somehow compensate for your lack of evidence. All it does is obscure your meaning.
If you are suggesting that because the burden of proof is on antivaxxers to prove skeptics are pedophiles, analogously the burden of proof is on skeptics to prove “those facts and techniques that have been exiled to the CAM tent” unsafe or ineffective, then you have grossly misunderstood the scientific method.
The blog consistently mangles that last link. I'll try again with this.
I mention vitamin C because it is the best documented dispute and most familiar. I don't know the Kansas U status or story. Sorry. Politicization strikes legit CAM experiments frequently, like the FDA's attack on vitamin C injectables shut down approved trials...
Moertel made conclusory statements about vitamin C that he was missing at least two orders of magnitude of data for the vitamin C blood levels e.g. 10 grams oral/day vs 200 grams IV in 2-3 hours. Moertel needed a **lot** of data for such sweeping negative statements. Moertel also was missing roughly an order of magnitude on treatment duration vs Pauling's data. There were a number of other discrepancies that Moertel et al indulged in.
These actions alone would demonstrate Moertel et al as biased quacks, scientifically.
Oh Krebs, damn you to hell Krebs! [shakes fist into the pelting rain]
Now I have to read the whole fcuking site. Thought they were busy and prolific for years, the Crofts activities on the internet seem to end abruptly in 2006. Were they picked up by Sylphs? Killed by Chemtrails? Secreted away by the NSA/CIA/NWO? Are they in the Rothschild's basement polishing silver, or are they in one of Lord Draconis' horrifying Paté Camps, tied down and forced to watch endless loops of Masterpiece Theatre™ whislt being force-fed a glop made of Cap'n Crunch and Guinness so that their livers will pop, thus producing lovely canapés for our Scaly Overlords™?
If you Google "Radithor" and go to its Wikipedia page, then follow the citations, eventually you'll come to a link to a newsletter in which is contained a reprint of a Wall Street Journal article with what may be the best headline ever printed:
The Radium Water Worked Fine Until His Jaw Came Off
I just had to share that.
If you google "Osteonecrosis of the jaw" and go to its Wikipedia page you'll find a modern iatrogenic epidemic of jaw breakdowns.
The Radium Water Worked Fine Until His Jaw Came Off
Now you you can do that with a nice choice of FDA approved bisphonates, all in the safety of your own home. If this jaw dropping event fails to impress and titillate all, one can try for sympathy with crutches. Break a leg ! (or femur, as the [legal] cases may be)
...irreversible see also PMID: 21138208 and 23370011
Quoting from Krebiozen above: You have a habit of writing in a curiously over-erudite manner, as if convoluted language might somehow compensate for your lack of evidence. All it does is obscure your meaning.
Quite possibly the best summary of CAM sophistry I've read yet on this blog.