
The reason there wasn't a post yesterday is simple. The night before, I was feeling a bit under the weather. As a result, I went to bed early, neglecting my blogly responsibilities. As I result, I missed the release of a whopper of a study that normally would have been all over like...well...choose your metaphor. On the other hand, the one day delay isn't necessarily all bad because it lets me see the reaction of cranks to this study, the better to apply some not-so-Respectful Insolence to it. The crankiest of these cranks, of course, is Mike Adams, a grifter deep in the thrall of any form of pseudoscience that he can sell to burnish his brand and keep the rubes buying and who knows how to whip his minions into a fine frothy head of anti-pharma conspiracy mongering. In actuality, though, I was a little bit disappointed, as Adams was almost restrained, at least by his usual crazed standards:
A CDC-funded medical study being published by the medical journal Vaccine has confirmed a shocking link between flu shots and spontaneous abortions in pregnant women. The study was rejected by two previous medical journals before Vaccine agreed to publish it, further underscoring the tendency for medical journals to censor any science that doesn’t agree with their pro-vaccine narratives.“A study published today in Vaccine suggests a strong association between receiving repeated doses of the seasonal influenza vaccine and miscarriage,” writes CIDRAP, the Center for Infectious Disease Research and Policy.
“A puzzling study of U.S. pregnancies found that women who had miscarriages between 2010 and 2012 were more likely to have had back-to-back annual flu shots that included protection against swine flu,” reports Medical Xpress, a pro-vaccine news site that promotes vaccine industry interests. Notice that the opening paragraph of their study assumed the study couldn’t possibly be true. It’s “puzzling” that mercury in flu shots could cause spontaneous abortions, you see, because these people have no understanding of biochemistry and the laws of cause and effect.
Actually, as has been documented so many times before, it is Mike Adams who has no understanding of biochemistry—or any other science—other than what it takes for him to portray himself to his gullible followers as a "real scientist." As for the "laws of cause and effect," whenever someone says something like that in reference to an epidemiological study, I know he's really, really clueless, because if there's anything that's very difficult to do in an epidemiological study with reliability it's determining cause-and-effect. That's why the cardinal rule of epidemiology is that correlation does not equal causation. It might, but usually it doesn't, and it usually takes a whole lot more than just one study with a correlation to start to suggest causation. This is particularly true when a study like the one Adams is gloating about is such an outlier, which this study most definitely is, as you will see. It's also an exercise in data dredging that illustrates the danger of small numbers in studies like this.
Let's go to the study itself. I can't help but note that Frank DeStefano of the CDC is a co-author. DeStefano, as you might recall, is one of those CDC investigators that antivax conspiracy theorists like those who made the propaganda film VAXXED portray as one of the main villains in the "CDC whistleblower" conspiracy theory. Also, several of the authors receive pharma money for research support. Nicola Klein, for instance, receives research support from GlaxoSmithKline, Sanofi Pasteur, Pfizer, Merck, MedImmune, Novartis, and Protein Science, while Allison Naleway receives funding from GlaxoSmithKline, MedImmune, and Pfizer. Others receive support from MedImmune and Novavax. So basically, this was a study funded by the CDC and carried out by CDC scientists and scientists receiving significant pharma funding. I just couldn't resist pointing that out. I know, I know, antivaxers will claim that the findings were so compelling that not even the CDC and pharma shills could hide them, but it would amuse me to point these things out to antivaxers.
Yet, here we see Del Bigtree, producer of VAXXED, gleefully citing J.B. Handley gloating over this study:
Tough breaking news for @ChelseaClinton @DrPanMD @doritmi FLU SHOT linked to MISCARRIAGE! #endvaxinjury https://t.co/6JwjnsAviY
— Del Bigtree (@delbigtree) September 13, 2017
I wonder if he knows that DeStefano is a co-author. He probably doesn't care, because DeStefano, like any scientist, can be a hero or a villain depending solely upon whether he produces information or studies that agrees with the antivaccine narrative that the flu vaccine is not just useless but dangerous. Be that as it may, the article above is a typical bit of Handley's Dunning-Krugger arrogance of ignorance, even more full of hyperbole and nonsense than the usual Mike Adams' endeavors in that area. Indeed, Handley even uses the argumentum ad package insert gambit. (Whenever I see that gambit used by an antivaxer, my estimation of his cluelessness goes up several notches, which for Handley is really saying something.) In any case, you can get a feel for how much the authors of this study are stretching to find a correlation—any correlation—between influenza vaccines and miscarriages that they're looking at combinations of vaccines by their brief justification for the study:
Since 2004, the Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices (ACIP) and other organizations have recommended routine influenza vaccination for pregnant women regardless of gestational age [1,2]. Influenza in pregnancy can cause serious, life-threatening illness in both the mother and fetus, as demonstrated during the 2009 pandemic [3,4]. Numerous studies of influenza vaccine during pregnancy have not identified serious safety concerns [5–12], but relatively few investigations have evaluated vaccination in the first trimester, a period when the embryo is highly vulnerable to teratogens and other factors [5,13]. A case-control study conducted by the Vaccine Safety Datalink (VSD) demonstrated that influenza vaccination during early pregnancy in the 2005–06 and 2006–07 influenza seasons was not associated with spontaneous abortion (SAB) [14].
The emergence of a pandemic influenza virus, A/California/ 7/2009 (H1N1)pdm09 (pH1N1), led to rapid development and widespread use of vaccines containing pH1N1 antigens. Several studies have evaluated the safety of vaccines containing pH1N1 in pregnancy, but few have focused on outcomes in early pregnancy [15–19]. Using a design and protocol similar to the previous study [14], we conducted a case-control study to determine if receipt of influenza vaccine containing pH1N1 was associated with SAB.
Notice the eight studies cited (references 5-12) that failed to find significant safety issues with the vaccine in pregnancy, and a study (reference 14) using VSD data failed to find an association between flu vaccination with spontaneous abortion. That's actually a lot of data for the safety of the flu vaccine during pregnancy, which makes me wonder what the justification for yet another study looking for an association between influenza vaccination and miscarriages. If I were a funding agency and received a grant application to do a study like this with text above in the "Background and Significance" or the "Impact" section, my first reaction would be: Why on earth would we fund this? It's all been done before, many, many times. Yet the CDC funded this study. So much for antivax claims about the CDC not being concerned about vaccine safety and not being willing to look for adverse reactions due to vaccines.
I also find it rather odd that the authors would say that few studies have been done looking for a correlation between vaccination against influenza, when in fact there have been a lot, many well-designed, and they've pretty much all been negative. Whenever you see a study that finds something a lot different from the bulk of the studies that have been done before, the first question to be asked is: Are the results of the current study so robust that they indicate a hole in the existing data addressing the question asked that we should begin to question the cumulative results of all the studies that have gone before? Keep that question in mind as I continue.
Also consider the bias that exists in journals to publish novel findings. As this news report points out, this is the "first study to identify a potential link between miscarriage and the flu vaccine." That's almost certainly the reason that it was published. Adams, in his haste to portray as a conspiracy to silence, inadvertently tells me something. That this paper was rejected by two previous journals is not surprising to me. What is surprising is that Vaccine ultimately accepted it. Of course, how Adams would know that this paper was submitted elsewhere and rejected, I don't know, which is why I have my doubts about Adams' claims.
So what about the study itself? First, it's a case-control study. Basically, that means that the authors found a cohort of women who had miscarriages (the cases) and compared them to a cohort of women who didn't have miscarriages but instead delivered full term infants or had stillbirths during the study period (the controls). The authors chose two flu seasons (2010 to 2012) and asked if women who had miscarriages were more likely to have been vaccinated for influenza within 28 days prior to miscarriage, as well as for different time periods before miscarriage.
The most critical aspect of any case control study if, of course, the matching of cases to controls. The idea is to match them as closely as possible on all relevant factors other than the condition under investigation (in this case, miscarriage). Not uncommonly, investigators will do a 2:1 match, controls to cases, in order to make the comparison more robust. It's not mandatory, and Donohue et al chose not to do this. In this study, cases had SAB and controls had live births or stillbirths and were matched on site, date of last menstrual period, and age. I also note that the database they used was the Vaccine Safety Datalink (VSD). As I like to say, the VSD is an excellent rebuke to antivaxers who claim that doctors don't care about vaccine safety. It's a database designed to document adverse events associated with vaccination, and it's a huge database. I've discussed it before on more than one occasion.
So what did the study find? Here's a summary of the cases analyzed:
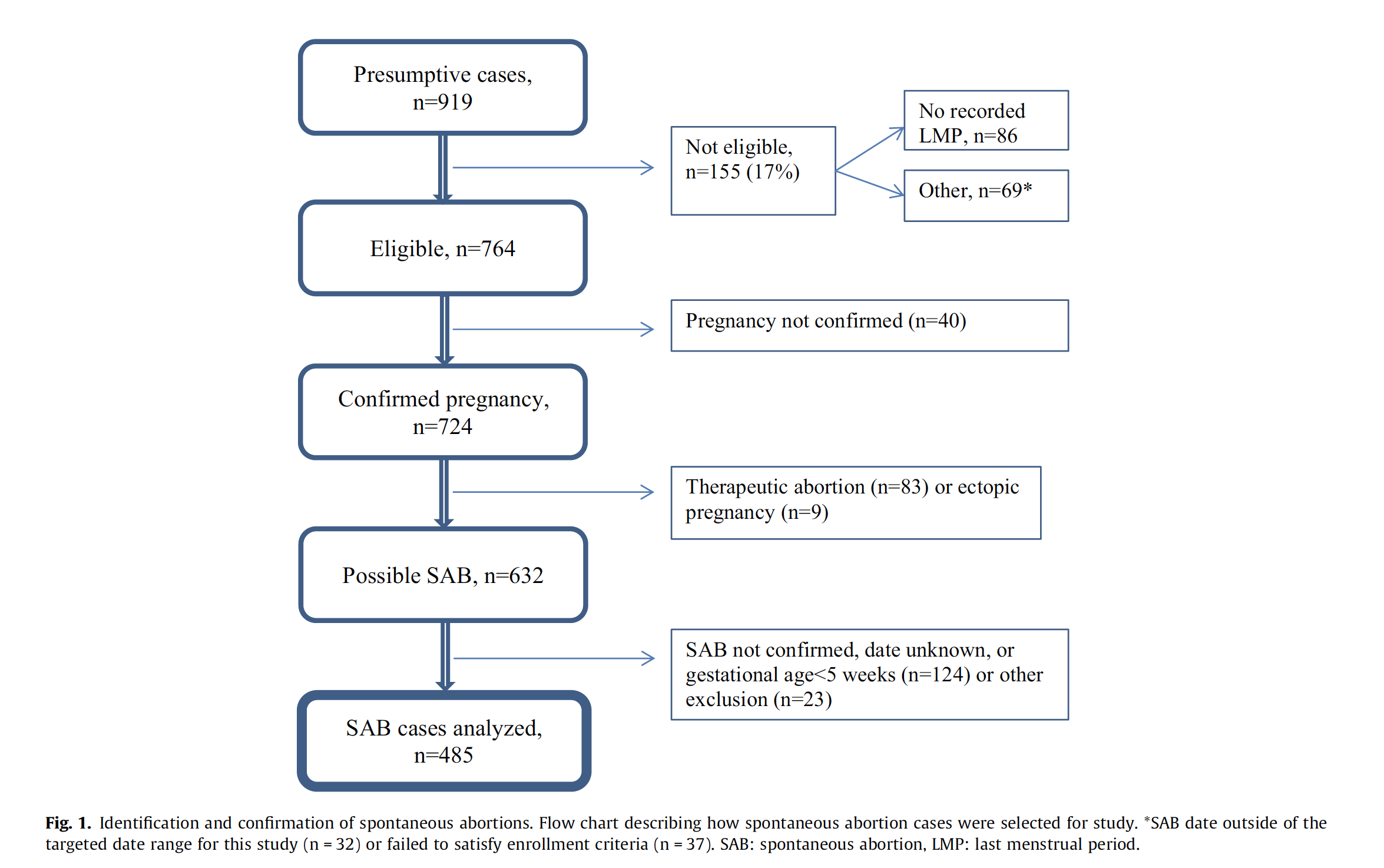
if you look at the tables in the paper, the first thing you will notice is that the adjusted odds ratios (aORs) for miscarriage as a function of having received the flu vaccine are nearly all around 1.0 or not statistically different from 1.0. Obviously, there are exceptions. Basically, the study found that, if a woman had consecutively received a flu vaccine containing the 2009 H1N1 virus the season before and had the flu vaccine in one of the two seasons studied, the aOR in the 1–28 days was 7.7 (95% CI 2.2–27.3). Otherwise, the aOR was 1.3 (95% CI 0.7–2.7) among women not vaccinated in the previous season; i.e., not statistically significant from 1.0, meaning no detectable difference in miscarriage rates compared to women who had not been vaccinated. This effect was noted in both seasons.
Now here's where you should be skeptical.
This study has several important limitations. First, the most striking findings relate to the association between SAB and IIV [inactivated influenza vaccine] in women who previously received pH1N1-containing vaccine. This interaction effect was not an a priori hypothesis; the results were generated in a post hoc analysis with small numbers of women in the various subgroups. Although the interaction was observed in each of the two seasons studied, the point estimates were substantially larger (though not statistically different) in the first season for reasons that are unclear. Second, although most cases had an ultrasound, assignment of a precise date of SAB was challenging. With guidance from an obstetrician we integrated different types of information from the medical record (e.g., ultrasound results, clinical and laboratory findings, provider notes) to estimate the timing of the SAB. Estimation of SAB dates was independent of vaccination status so any error should bias the results toward the null (i.e., non-differential misclassification). Third, we studied only women who had clinically confirmed SAB; the proportion of women with clinically unrecognized pregnancy loss is uncertain but may be substantial [50,51]. Our results could be biased if women who sought care for SAB were more likely to be vaccinated in the 28-day exposure window.
So what we're looking at is an association, nothing more. It's an association with a lot of caveats, too. Basically, having found nothing more than one association with an aOR of 2.0 for the 1-28 day window of exposure to the influenza vaccine before miscarriage that was barely statistically significant (95% confidence interval: 1.1-3.6), the authors did a post hoc analysis looking for other associations. (Never mind that the "association" they found was eminently unimpressive given the size of the confidence intervals.) "Post hoc" means that they did additional analyses not originally specified. Basically investigators don't usually do post hoc analyses if there is a robust association in their data. They do it when they fail to find an association or only find an unimpressive association that is not robust. Also, post hoc analyses are prone to type 1 errors, which means finding a statistically significant "association" where there is none; i.e., finding a false positive. When the numbers in the subgroup are so small and the study is observational (i.e., retrospective), that tendency is even stronger. Then there was the issue that the cases and controls were not as comparable as one would like in a case control study. For example, cases were significantly older than controls and more likely to be African-American, to have a history of 2 spontaneous abortions, and to have smoked during pregnancy. The authors did some correcting for age and history of spontaneous abortions, but it's questionable to me whether it was adequate.
Basically, the authors did what we refer to as a subgroup analysis, in this case the subgroup being women who had received H1N1 vaccination the season before they received the flu vaccination in the seasons examined? That clearly wasn't a primary hypothesis being tested. Rather, it was a hypothesis the authors clearly came up with while doing the study. One wonders if this analysis was prespecified or whether the protocol was changed midway through. I only ask that because antivaxers went wild over claims by the "CDC whistleblower" that the Atlanta MMR study changed its protocol part way through the study, but, here, where the analysis seems to suggest such an "adjustment" during the study (although it is certainly possible that the H1N1 analysis was prespecified in the original protocol, given the choice of the 2010-11 and 2011-12 flu seasons), we hear...silence. Whatever the case, there clearly was post hoc analysis strongly resembling p-hacking going on here, in which the investigators, having failed to find much, started looking at other potential associations. Certainly, it smells that way.
Speculations about the protocol aside, the investigators found what they found, namely an aOR of 7.7 for cases versus controls for exposure to the H1N1 vaccine the year before plus the flu vaccine within 1-28 days before their miscarriages. This was based on some very small numbers, though, namely 14 miscarriages and 4 controls. In other words, this is almost certainly a statistical fluke, given that it was only found for women who had received H1N1 the season before and had received the flu vaccine within 28 days of their miscarriage, and that the association was not observed for pretty much any other time window or combination. When considering such a result, one also has to consider biological mechanism and plausibility, and it is just not very plausible from a biological or immunological standpoint that this combination of flu vaccines—and only this combination—given only during a specific time window will cause miscarriages. Like Dr. Gregory Poland, the editor of Vaccine, I don't believe these findings, either.
I particularly don't believe them in light of what we already know, based on studies Tara Haelle summarized the data with respect to flu vaccines and miscarriages, stillbirths, and birth defects in 2014, using mainly studies published during the prior two years, and the results were very consistent and overwhelming: There was no association between vaccination for influenza and adverse fetal outcomes. Just for yucks, I did some PubMed searches myself for more recent studies, and found basically the same thing, but instead of listing those studies, I'll just refer you to a recent large meta-analysis that found that the risk of stillbirth was actually lower in women vaccinated against influenza and no difference in the risk of spontaneous abortion. In other words, this new study is an outlier. It's such an outlier, that scientists are correct to be very skeptical of its results. Heck, even the authors are skeptical of its results. Unfortunately, they're not so skeptical that they don't resist making the call for "more research." They'll probably get the funding for that "more research," and then when the inevitable negative study is finally published, no one will remember it. They'll all remember this study, and, of course, the antivaccine movement will be flogging it for years to come.
Me. Adams seems to have taken the point about two rejections from this article. Which did a reasonable job at pointing out the nuances, though without your more in depth analysis of the science.
https://t.co/qBGRBZKaJk?amp=1
And just to add, miscarriage can certainly follow H1N1 infection. https://www.ncbi.nlm.nih.gov/m/pubmed/21345415/
Thanks you for this review. As I suspected, the confidence intervals include 0 in which one with a basic understanding of statistics would realize the association is more likely due to chance and therefore is not significant.
Anti-vax sites are already spreading this as "evidence" for the evils of the influenza vaccines. Yet one would have to believe a sub-group analysis of a tiny group of patients(which is prone to bias and error as mentioned above) over meta-analyses with much larger number of patients which reveal the opposite trends. This is an immense error in deductive reasoning and is a classic example of "cherry-picking."
As a retired epidemiologist, according to my education, training and experience, post hoc analyses can only be used to generate hypotheses to be possibly tested in additional research which is exactly what the authors concluded with: "This study does not and cannot establish a causal relationship between repeated influenza vaccination and SAB, but further research is warranted." I guess Mike Adams and the gaggle of morons at Age of Autism missed this part.
However, as you said, the sample size was too small, as can also be seen by the wide confidence intervals. In addition, as the number of analyses of any research increases, multiple comparisons, the risk of "randomly" finding something significant increases. So, given the strength of the already existing evidence, I disagree, as you do, with the authors that "further research is warranted."
Typical also of antivaccinationists is downplaying the risks from the actual disease: "Certainly the risk is far worse than the sickness." (Yesterday's article, Flu Vaccine and Miscarriage, in Age of Autism). I guess in their minds that getting flu while pregnant doesn't pose a risk. Sometimes, when reading them, I ask the question: "What planet are they from?"
I don't recall where I read it, but didn't the group with more miscarriages have women at higher risk, anyway, than the controls? IIRC, there were more smokers, older women, diabetics in that group. And they are statistically more likely to miscarry anyway. (If I wasn't working, I'd go search my home computer for the item).
Dawn, it was included in a comment I made yesterday, quoting from this source -
http://www.cidrap.umn.edu/news-perspective/2017/09/study-signals-associ…
I'm in my first trimester and I'm getting my flu shot.
Thanks, Johnny!
Refresh my memory here: is the VSD the database that includes a rather generous definition of vaccine-associated injuries, or is that some other database? Because if it is the database I am thinking of, then the failure of earlier studies to find an association is especially damning, given that database's bias toward overreporting adverse reactions to vaccines (which presumably would include miscarriage).
So it's another case of picking out the one outlier and deciding that it must be proof of absolutely everything evil they believe about vaccines?
And of course that's without even bearing in mind that people who get flu vaccines are more likely to have health conditions that put them at greater risk of miscarriage to begin with, such as smokers, asthmatics, people with COPD, people with heart disease, advanced maternal age, etc.
To Adams, of course, rejection by two journals is evidence of a conspiracy. To the rest of us, it's reason to ask why the paper got rejected twice. Since the paper gave a whisper of evidence that he desired, he skipped that question and just went straight for the conspiracy theory.
The obligatory XKCD on statistically significant outliers: https://xkcd.com/882/
I'm throwing this study out to the epidemiology students to see who can point out the most sources of bias and confounding. I would say that this a jump-off to more studies, but, truth be told, there is a lot of understanding of what the flu vaccine does for pregnant women at a population level: IT PREVENTS COMPLICATIONS FROM INFLUENZA. And that understanding comes from better studies than this one as well as observational studies gained from outbreak investigations.
Those sources of bias and confounding don't happen to include the older age, higher rate of smoking, and higher proportion of African-American women among the cases compared to controls, now would it?
I was actually wondering: Why is it that the investigators couldn't match their controls to cases better? Why didn't they do a 2:1 match, which could have decreased this problem?
Side note: JB Handley has blocked me on medium.com from seeing his posts... If I'm signed in. I've been very critical of his pseudo-science, and he seemed to have difficulties replying to the facts I've prevented. So much for transparency and open discussion. Then again, it's JB. He compared Wakefield to Jesus, so...
-A few days ago, AoA ran an article by Ginger Taylor which claimed that the CDC placed a ' gag order' on its employees so that they wouldn't speak to the media...
NOW WE KNOW WHY!!!1!
- TMR's 'Professor' O'Toole has been ranting against the AAP's position on Hep B vaccines at birth
-btw- TMR has much less posts recently.
- Just before the article quoted above, Mikey Boy fumed about celebrities' support of Planned Parenthood (which is solely abortion, in his mind).
Knowing Mike as I do I can imagine a parody he might write:
" Hello LADIES!
Are you bothered by one of those pesky unwanted pregnancies? Are you worried about the HIGH price of abortions over at BabyKillers, LTD?
Well, here at HexAll drugs, your local toxin pusher, we have a great solution for your problems! Get one of our flu vaccines and you can dodge both a minor illness and 18 years od caretaking all in one shot! **
** I know, I know my grammar is too good
Both Handley and Wakefield are legends in their own minds. So it makes sense for them to compare each other with a certain first century CE carpenter-turned-rabbi.
@Eric Lund #9, I think you are referring to the Vaccine Adverse Events Reporting System (VAERS). Vaccine Safety Datalink uses data from AVERS and other sources to monitor Vaccine safety.
https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/vsd/index.h…
"an aOR of 2.0 for the 1-28 day window of exposure to the influenza vaccine before miscarriage that was not statistically significant"
It was: "The overall adjusted odds ratio (aOR) was 2.0 (95% CI, 1.1–3.6) for vaccine receipt in the 28-day exposure window"
Or Gene Simmons, but even that's probably too charitable.
OK, Jake. Now explain to us all, as someone who *should* understand statistics, why that's not statistically significant. (Hint...I hated, loathed, despised stats and I can do it).
The text was originally intended to read "barely statistically significant," which is accurate. I have altered the text to be in line with my intent. When one writes blog posts in one's spare time late at night, such things occasionally happen; one occasionally makes mistakes. The difference between a certain Gnat and me is that I correct my editing errors.
In any event, "statistically significant" or not, given the very wide confidence intervals, the lack of robustness, and the differences between the cases and the controls in the frequency of known risk factors for spontaneous abortion (the cases being older, more likely to smoke, and more likely to have had a history of >2 spontaneous abortions) the association reported is eminently unimpressive. Hmmm. I think I'll add some text very much like that to the post. :-)
My only comment today is going to be this: To all Orac minions a virtual cigar. My Daughter was born at about 6am PDT in Chiang Mia. She is healthy and weighed 6.2 lbs and was 19 inches long.
Everyone have a very good day; I am going to.
Rich
Mazal tov!!!
Congrats!
Congratulations Rich, but please keep those cigars very far away. I really hate that smell.
Renate, that is why I said virtual cigars. I don't like them myself.
Thanks Dorit
Congratulations, Rich! Honored to share a virtual cigar with you.
@MI Dawn:
I won't, because it is statistically significant. Orac is wrong and should retract.
Congrats, Rich! May you know much joy in your daughter. They are wonderful things to have (I know - I have 2 of them.)
@Jake: barely, as Orac noted. My stats prof (to whom I showed this) said I was wrong, it is statistically significant. And if I tried to use such a wide CI and pass it off as significant, she'd mark me wrong unless I noted it was barely significant, as Orac noted above.
And hey, unlike you, I can actually admit it if I'm wrong. Provided I ask people whose opinion I respect, and who point out my errors honestly.
Amusingly, The Gnat has nothing to say about the rest of my discussion, particularly the part about the post hoc subgroup analyses. If there's one thing physicians are appropriately taught about statistics, it's to distrust post hoc subgroup analyses.
That is an error (which seems to derive from CIDRAP; they will eventually fix things if E-mailed), but you're also grasping at a single clause while missing the point, which is that there's no reason why two specific seasons would amount to something when neither does on its own. (P = 0.03 on that CI, for those scoring at home.)
I think I was confusing a passage for individual seasons with the combined seasons, which explains the text slip. Oddly enough, I looked at my saved versions in BBEdit and saw that I originally had it right, then for some reason in an edit it changed. Ah, well. I stand by what I said about its being "barely" statistically significant, and I also note that robustness is important. This finding just isn't robust. It barely achieves statistical significance, and only then for one analysis. That's the sort of result that screams false positive.
There is nothing magical about using p<0.05 as a threshold for statistical significance. It is frequently done because there are many fields where one rarely has enough data to use a more stringent criterion, but the downside is the danger of false positives. Remember that if you are drawing data from something that has no correlation, you have a 5% chance of your sample producing p<0.05. See the obligatory XKCD link.
That's even before we get into issues of systematic bias, which statistical tools generally don't handle well. The assumption is that the case group and control group are equally likely to suffer an adverse result in the absence of whatever intervention you are testing to see if it changes the risk. It sounds like the case and control groups here are not well matched, such that one would expect a priori that the case group would have more miscarriages than the control group. When that's the case, you shouldn't be surprised that the case group actually does have more miscarriages.
So no, Jake, Orac is not wrong to say it's not statistically significant, just because it barely meets an arbitrary threshold.
Heheh. Thanks. I'm aware of all these issues, of course, but didn't see this post as the place to discuss them. For instance, in the context of discussing John Ioannidis' work, I've pointed out on at least a couple of occasions that setting the threshold for statistical significance at p≤0.05 means at least a 5% chance of a false positive but that it's actually a much higher chance than that, even in randomized clinical trials, due to undetected biases and shortcomings in carrying out the studies. In retrospective studies like this one, it's higher still. In post hoc subgroup analyses, it's the highest of all.
Thanks, Rich, but I will pass on the virtual cheroot, and instead hoist an actual adult beverage this evening in honor or the young Miss Bly.
How's your batting average with that routine lately, Jake. It might be time to outgrow amounting to basically just being a whiny little shit.
There is that, but there is also the point that a small p-value is not any evidence against your null, as its calculation is based on the null being precisely true.
The original intention of a small p-value was that it was a signal of something that might be worth further investigation. We (statisticians) got off course when Neyman and Pearson ritualized classical hypothesis testing, and the teaching of p-values and their meaning has been generally poor ever since.
And -- there is no a single bit wrong with Orac's take on the "significant" result here (as he knows, others know, and anyone who claims to understand statistics and is honest should know).
Congrats Rich!
May Baby Bly long continue to be healthy and happy...
I have a virtual cigar joke, but I'll leave it to the minions' imaginations. :-)
For those of you seeking a moment of comic relief, Levi Quackenboss suggested that this was published by the media - who, in her world, is of course controlled by pharma (that's why they didn't publish articles when flu mist was shown ineffective, or about the problems with mumps vaccines, and so on - oh, wait) because a universal flu vaccine is nearing completion.
https://leviquackenboss.wordpress.com/2017/09/14/why-is-the-media-attac…
I don't think she's joking, even though it reads like satire to me.
@ Jake:
Too bad you don't understand what statistical significance actually means or how it differs from clinical significance. Quite simply, if one were to randomly sample from the same population an "infinite" number of times, based on known probability distributions, one can estimate the probabilities of various outcomes, e.g. only 5% of time will a certain outcome occur and, assuming that the sampling and, in the case of a case-control study, the matching, was well done, then one assumes that the outcome relates to the hypothesized variable(s); but 5% of the time the outcome could have been brought about by variables not controlled for/random chance, regardless of how well the study was done. However, it is an artificial cut-off point for decision making and in this case as the matching was poorly done, the sample size small, it was a post-hoc analysis subject to multiple comparison problems in deciding statistical significance, and there are numerous well-done studies that do not agree, it is meaningless. But, given your rigid bias, whatever even remotely fits your ideology becomes significant.
I find it hard to believe that you were accepted in a doctoral program at the University of Texas School of Public Health; but, then again, over the years I've met people who managed to learn things and pass exams without really understanding them.
I suggest, to start with, you read the following:
Merwyn Susser (1973). Causal Thinking in the Health Sciences: Concepts and Strategies in Epidemiology.
Any bets on how long it will be until some random gibberish about original antigenic sin starts making the rounds?
That's a sucker bet....
The Gnat should go back to his self-copulatory Milo fantasies.
Congratulations on the birth of your daughter, Rich!
That one big finding wasn't even 17 cases and controls. It was 14 cases and 4 controls! Four! This is just an astoundingly weak study and I wonder why DeStefano keeps doing these kinds of post hoc subanalyses.
I'm also not convinced they controlled adequately. Their matching was very poor. Age groups (+/- 30 years) are far too broad. Matching by region does not account for variation within regions. If cases are more likely to be African-American, they're more likely to be worse on SES measures. I'm in one of these regions and I can tell you that we are so segregated, a random sample of AAs and whites would not be remotely comparable.
I'm glad someone posted the jelly bean comic. That's on the outside of my cubicle wall, which I put up there after the "whistleblower" brouhaha. So much irresponsible science.
If you torture any dataset enough with post-hoc/subroup analyses, eventually it will give you an answer you want to hear.
But like all other forms of torture, that answer is rarely correct.
To those of us at the coalface, diagnosing, treating and attempting to prevent life-threatening vaccine-preventable diseases, studies such as this are never considered clinically applicable.
@ Joel A Harrison, PhD, MPH:
Thanks for attempting to educate Jake:
Lord knows, I tried and got nowhere. But it showed his bent.
Seriously, he should have got stat basics years ago and he didn't. Needless to say, he is clueless in other ways. As well as resistant to new info/ reality.
I would hope that other minions would chime in too. Like when people do an intervention: many voices saying the same thing in diverse ways.
Well, he's not there anymore. According to Jake's "About" page on the White Rose and Hans Litten blog: "He was dismissed from the Ph.D. Epidemiology program of the University of Texas School of Public Health, due to academic misconduct by the school’s administration."
But I digress...
Yes, one of the things that academic epidemiologists keep getting wrong is translating their findings into meaningful action/practice/policy. The first thing you ask when presented with any finding is, "So what?" Then you tease it apart.
In the case of this study, I'd ask, "So what? Actual influenza causes way more death and disability, and miscarriages, in pregnant women than the vaccine would if this study were valid." Even the authors of this study, the editors of the journal, and everyone worth their salt (and not kicked out of a doctoral program in epidemiology) have pointed out that this is not a finding on which flu vaccine policy/recommendations in women should be changed. I'd take it a step further and ask why, oh why did they publish this?
As Orac pointed out, a matched case-control study would have been stronger. One-to-one like this, and if you draw them from a similar population, you might control so much that you stratify on a collider and get a whole new bias in there. (We saw this when they drew cases and controls from the same medical setting for the coffee-pancreatic cancer study back in the day.)
These are very complicated issues to understand in epidemiology, so you really can't blame the public for now getting confused over this. Now, we are going to have to go get a more robust study done to explain the association seen in this one, which is a waste of time and resources. And you're going to have women who will choose to forgo the influenza vaccine in what promises to be a very active flu season if the "as Australia goes, we go" rule kicks in this winter.
@ Ren:
Wow, thanks for the info on Jake being kicked out of doctoral program. After I finished my PhD at the University of Gothenburg in Sweden, I received a post-doctoral fellowship from the National Institutes of Health in a program at the University of Houston, applying social psychology to preventing cardiovascular disease. As part of my training, I took at MPH and then an MS in biostatistics and epidemiology at the UT School of Public Health in Houston. I still have friends there 35 years later; but, Jake was at the UT Austin campus. Still, it's a good school and hard to believe he ever even got into the program.
And I do remember the coffee-pancreatic cancer study, published in the top journal, New England Journal of Medicine if I recall.
By the way, even if there was a rare chance of the flu vaccine contributing to a miscarriage, though there isn't, full blown flu in the first trimester would affect far more with devastating consequences. As I mentioned above, antivaccinationists, thanks to vaccines and never having seen the results of the vaccine preventable diseases, downplay the risks from them. I remember kids with iron braces and one in an iron lung. Not memories I cherish and I was in first cohort to get the Salk vaccine in 1955.
I believe MI Dawn may have touched on this and I am probably veering horribly outside my lane, but wouldn't women with a prior history of problem pregnancies (including miscarriages) be more likely to also be getting flu vaccines? I would think their physicians would strongly recommend it as part of a regimen of risk reduction.
I'll return to betting whether I can persuade the niece and nephew to eat bell peppers stuffed with sauteed garlic chicken livers, black beans with feta. My guess is not. There's a reason for that bag of chicken nuggets in the freezer.
due to academic misconduct by the school’s administration.
Roughly translated: "Failure to recognise my genius and originality".
Where do you get garlic chickens?
Oh man, that sounds good. My host granny in Russia used to make chicken livers with some kind of garlic sour cream sauce and serve it over buckwheat. I love that.
I have a few things planned: chana masala, fattoush with homemade Arabic bread, a spicy Palestinian shrimp recipe. Jambalaya for company at some point after this part of hunting season is over (my brother has been requesting it.) Plus I'm sure typical stuff like pizza and some sort of meat-and-potatoes.
I hear you on the nephews. I made a bunch of Palestinian food a while back and, well, at least they liked the bread and the rice-and-vermicelli pilaf.
Honestly, my brother can be almost as much of a challenge sometimes.
I mean, if we're going to devolve to talking about food... :-)
M'judra/mujaddara is a pretty popular comfort food; the Palestinian fellow at the Cornell Dollar says his kids love it.
@ JP #52
Like most kids, they sometimes have a limited view of what foods they will even try. Unfortunately, at ages of about seven and six for the niece and nephew, we and their parents made a few mistakes on a vacation - raw oysters, fresh lobster, mussels, and softshell crab. Do not, I say again, do not give children the chance to acquire expensive tastes. We thought the texture of the oysters would put them off and the others would be too strong a flavor. We were very wrong and they could both pack those items in like harvest hands, given the chance, even at those few years. Do you have any idea how embarrassing and unseemly it was to squabble with a seven-year-old for my fair share those things at my age?
/thread hijack mode off
This did at least elicit a Gerg classic, in which he apparently accidentally throws Thompson under the bus.
@Rich Bly,
Congrats and hope the mom & baby are doing well.
More on Mike ( Natural News, yesterday):
Not only do vaccines cause miscarriages but they complement a covert depopulation plan involving spiked foods as well as other vaccines' dire effects, Planned Parenthood's focus on aborting non-whites and other monstrous atrocities.
He read it in the NYT ( 1969 article quoted)
I couldn't find a copy of the entire paper (for free), so I've just read the abstract. It's not clear from reading the abstract whether the authors adjusted for procedures known to increase SAB, such as amniocentesis. Additionally, given the short interval of follow-up, it seems like a cohort study would have been a much stronger study design.
So Jake is right for once, and, as you would expect, he handles it with all the grace and composure you would expect.
http://www.autisminvestigated.com/david-gorski-vaccine-miscarriage/
I've a comment in moderation, and I expect that y'all will say there is too much expectation for such a simple post. Don't expect me to disagree.
Can a brother get a preview button up in this place? Or am I expected to just scroll back and re-read what I type to see if it meets my own expectations? I expect I know the answer.
I don't know if it does cause flu vaccines, but all I know is that all the good chemistry jokes argon. ?
https://m.facebook.com/pg/3MPhilippines/posts/?ref=page_internal&mt_nav…
I suspect that, in your heart of hearts, you already know the answer to that question.
@ Johnny:
Thanks for that link.
I think Jake is attempting to rescue his self esteem after being booted... I mean DISMISSED from UT:
-Notice that he himself found an error which Orac, PhD MD and two epis ( PhD Joel and PhD C Ren) missed.
- he includes a video of his triumphant ( heh) debate with Orac.
- he introduces Orac in Mike Adamsian fashion
- he grandiosely refers to himself in the third person as editor
- and didn't get the point of what Orac and commenters wrote
A few years ago, just prior to his study at GW, I warned him that his web activities and woo positions might doom his chances at a career in SB professions.
So I suppose I was right:
he won't ever work legitimately and has to be content editing/ writing a childish web project whilst pretending to be both a journalist and a scientist.
His family has enough money that he may eventually become a film maker *a la* AJW or Gary Null or even hit the big time with a web scandal sheet like dear old Mikey or Bolen .Maybe he'll write an expose tome published at Skyhorse.
BUT like Kim and Mark and others at AoA, their 'careers" don't exist outside a very narrow internet niche of partisans.
Do any of them teach anywhere? Or work as reporters? Or have clients/ patients**? I don't think so.
** Unfortunately, some real woo-meisters do have clients who pay for quackery. Not a goal anyone should aspire to.
I didn't bother to look at The Gnat's little tirade; so thanks for the summary. (Why waste time and brain cells, after all?) I used to feel sorry for The Gnat because he's just so damned pathetic, but over the last couple of years, his complete embrace of the alt right (including its racism and misogyny) along with his continued embrace of antivaccine pseudoscience (not to mention his general nastiness) has led me to cease to have any sympathy or empathy for him. He's just not worth it. He's an adult; he's made his choices; and those choices are, by and large, despicable.
I'm sure The Gnat's little rant will soon find its way to Natural News; that's how low The Gnat has fallen.
This sentence is also wrong: "Basically, the study found zero (that’s right: zero, nada, zilch) association between miscarriage and flu vaccination—with one exception: if the woman had consecutively received a flu vaccine containing the 2009 H1N1 virus."
Hmm. I hear The Gnat buzzing again. Amazing how he focuses in on one single sentence. It's certainly because he can't deconstruct the whole post or otherwise show why this study's result is not a statistical fluke when even the authors of the study admit that it almost certainly is, even as they ask for more funding to do a followup study. To humor The Gnat, I deleted that sentence, which was a holdover that I forgot to delete the first mistake.
That's because, unlike The Gnat, I am intellectually honest.
Orac talks about how JC "focuses in on one single sentence" and " can't deconstruct the whole" :
believe me there's a name for that but I'm not allowed to say that / too much like a diagnosis.
Now that Jacob Crosby, MPH, has been expunged from the Ph.D. program at the University of Texas I suppose that he, as an advocate of accuracy in media, will have many hours available to correct the misstatements that he has promulgated.
Indeed, as Narad suggested, it might be time for Toxic Boy to update his readers on the expected publication date of the Proceedings of the National Academy of Sciences article in which, Crosby claimed, William Thompson would (in May 2016!) repudiate his statements that MMR was associated with an increased risk of ASD in a subset of African-American boys because Thompson was bribed with a “huge bonus” and the promise of “his own autism research foundation.” Etc.
Orac (#67) writes,
I am intellectually honest.
MJD says,
And intellectually adaptive.
I really appreciate the picture you used at the beginning of this post.
You could have used this dreadful image from Naturalnews.com
http://www.naturalnews.com/gallery/640/Medical/Background-Vaccine-Latex…
"That’s because, unlike The Gnat, I am intellectually honest."
There is that. There is also the fact that you have an understanding of statistics, which he does not.
Jake has always had delusions of adequacy, stretching back to his AoA days. Sure, the rise of Orange Thinskin brought out a bit of a darker side in the lad. But I haven't noticed any changes in his posts after his departure from UT to suggest that it had that big of an effect on him.
DW, I love you like a sister, and you're right, you did warn him. But that's like predicting that the sun will come up in the morning - it didn't take any real skill. Everybody knew he was torpedoing his chances for any real job in the science or health industry, and his current on line activities, much like Captain Sockpuppet, will limit his employment in about any other job.
Of course, while everyone knew it, you did try to honestly warn him, and that counts for something. I also remember that he dismissed your warnings.
Some people learn from others. Some people have to pee on the electric fence for themselves.
The question is, will mommy ever get tired of giving him handouts? Will he ever realize that he's never earned a thing for himself? Will he ever think that (after what? 30 years?) 'maybe I should be able to live on my own'? Mommy and daddy have bought him a fine education (fine credentials, anyway), and he should be at least filing his own income taxes, not being carried as a dependent. But other than maybe earning a few hundred cross posting his 'work' at Epoch, he's never mentioned having a job.
Someday, that might bother him. Or not. He might be happy being a sponge.
That would be DrPH C Ren. Unlike the PhD types -- with all due respect -- I'm not too interested in academic research. I'm more about taking that research and putting it into practice... If I finish. The thesis has taken a life of its own.
Maybe I should keep it simple?
I note that Jake has let a post by the lovely and talented Rebecca Fisher appear under her own name. I believe it's the first in quite a while that he hasn't edited to change her name to 'Brian Deer'.
http://www.autisminvestigated.com/david-gorski-vaccine-miscarriage/#com…