

Seven years ago I returned to Michigan, where I was born and spent the first quarter century of my life, after an absence of more than 20 years. In the interim, I had done my surgical residency and earned my PhD in Cleveland, a surgical oncology fellowship in Chicago, and worked in New Jersey at my first academic job for eight and a half years. Then I was lured back with a job in Detroit. One of the odd things about this return after such a long absence was the culture shock, how much I had forgotten about the Detroit area. One of those things that I had forgotten is just how crazy about hockey Michigan, in particular Detroit (meaning the Detroit metropolitan area), is. Detroiters love their Red Wings—love them. Hockey is ingrained in the suburban culture from a very young age, so much so that many Canadians would feel right at home here. Memories of trying and failing to be halfway decent at street hockey and of not being anywhere good enough a skater even to try real hockey as a teen came flooding back to me. (It didn't help that back then I was approaching six feet tall and weighed only 135 lbs.; "beanpole" didn't even begin to describe me back then.) In fact, the "cultural center" of the town where I live consists of—I kid you not—a hockey rink and some classrooms and meeting rooms that are used for various community functions. No, really, its official name includes the words "cultural center.
So it should be no surprise, given how much Detroiters love hockey in general and their Red Wings in particular that it was big news here in late October when Red Wing legend Gordie Howe at age 86 suffered a debilitating stroke that paralyzed the right side of his body, a condition known as hemiplegia. Understandably, there was an outpouring of good wishes for recovery, coupled with retrospectives of Howe's stellar hockey career. Indeed, I remember that Howe's condition sounded bad enough from the tenor of the news reports at the time that it seemed likely that he would not survive. But survive he did, and has been apparently recovering slowly, with occasional setbacks.
Then, two weeks ago, I saw headlines all over the place that were basically similar to this Detroit Free Press headline, "Gordie Howe underwent stem cell clinical trial in Mexico." The story consisted largely of a press release from Howe's family that read describing Howe's "miraculous" rebound after having received a stem cell treatment in Mexico. As you might recall at the time, it was noted that there were saw a lot of holes in the story. It turns out that over the last week there have been developments that allow me to fill in some of those holes. Unfortunately, other holes still remain.
First, a brief recap is in order (You can click here for a more detailed timeline). Gordie Howe suffered a massive stroke on October 26, leaving him hemiplegic and with serious speech impairment. Since then, judging from various media reports, he has been slowly improving, although not without significant setbacks. We also know that Howe suffers from significant dementia. Out of the blue, a press release issued on December 19 by the Howe family announced that on December 8 and 9, Gordie Howe "underwent a two-day, non-surgical treatment at Novastem’s medical facility. The treatment included neural stem cells injected into the spinal canal on Day 1 and mesenchymal stem cells by intravenous infusion on Day 2." His response was described as "truly miraculous," although, as I pointed out in my post, it's not clear exactly what "miraculous" meant, given conflicting contemporaneous news accounts before the Howe family press release, particularly his hospitalization from December 1 to 3 for a suspected stroke that turned out to be dehydration.
Again, there were a number of problems with the story, the first of which was that Howe was clearly not eligible for the clinical trial offered by Stemedica, a company in San Diego that manufactured the stem cells used and was prominently mentioned in the Howe family press release. Another glaring issue was my inability to locate any description of an actual clinical trial for stroke offered by Novastem, the company that imports Stemedica's stem cells and runs Clinica Santa Clarita, where Howe received his treatment. I could find no such trial listed in ClinicalTrials.gov. Searching the registry maintained by the Mexican Federal Commission for the Protection Against Sanitary Risk (COFEPRIS) I was unable to find any registered clinical trials for stroke being carried out by Clínica Santa Clarita. What I did find were trials of stem cells for:
It all looked very fishy, as though Dr. Maynard Howe (CEO) and Dave McGuigan (VP) of Stemedica Cell Technologies, knowing that Gordie Howe was not eligible for their clinical trial for stroke (as detailed here), because Howe's stroke was less than two months old and the trial required that the stroke be six months old and that no neurologic improvement had occurred for two months, had shunted him to Novastem to be treated regardless. Looking at Novastem's website, in marked contrast to that of Stemedica. What I did see was (to me, at least) a very dubious-appearing stem cell clinic that charged patients large amounts of money to treat them with "stem cells," cash on the barrelhead. (Seriously, Novastem only accepts cash or money transfers.) With Christmas fast approaching, I did not expect to find out anything more about this story before the end of the year.
My expectation was upended on Christmas Eve.
In which I am sent a press release
On the afternoon of December 24, as I was preparing to head over to my aunt's house for our traditional Christmas Eve celebration, I received an e-mail from a woman named Kimberly Stoddard, who represents The Townsend Team, a marketing and branding firm representing Stemedica. Ms. Stoddard referred me to a press release entitled "Novastem Treats First Patient Using Stemedica's Mesenchymal and Neural Stem Cell Combination Therapy for Ischemic Stroke":
TIJUANA, Mexico, Dec. 24, 2014 /PRNewswire/ -- Novastem, a leader in regenerative medicine, announces the treatment of its first patient in its study for ischemic stroke at Clinica Santa Clarita. According to the American Stroke Association, ischemic strokes account for 87 percent of all stroke cases. Novastem continues to enroll qualified patients in the study, entitled "Internal Research Protocol in Combination Therapy of Intravenous Administration of Allogeneic Mesenchymal Stem Cells and Intrathecal Administration of Neural Stem Cells in Patients with Motor Aphasia due to Ischemic Stroke." All participants receive a unique, combination therapy using a method covered by a United States patent owned by Stemedica Cell Technologies for the therapeutic use of its allogeneic, ischemia-tolerant mesenchymal and neural stem cells.
My first reaction went along the lines of, "Well, that's odd. Who issues a press release like this on Christmas Eve? Nobody's paying attention now." My second thought was a speculation, "Well, maybe that was the point." My third question was whether this press release was a reaction to the skeptical posts about Gordie Howe's treatment with stem cells by Paul Koepfler and a certain party well known to this blog. In checking to see if Dr. Koepfler had written anything else, I found a follow-up post by him dated December 23 and entitled "Response from Stemedica on Questions on Stem Cell Treatment of Howe". It's not very informative, its only new information being that Stemedica didn't write the press release (its author was later revealed to be Gordie Howe's son Murray) and that "Stemedica is not a sponsor of the clinical trial referenced below; that is Novastem…"
And now we have Novastem and Stemedica's joint press release.
It was immediately obvious to me (and anyone else who had paid attention to the stories about Gordie Howe) that this first patient treated was, in fact, Gordie Howe, although the press release quite properly did not name him. One thing I wrote in my original post that this press release did confirm for me is that the principal investigator (PI) of this "trial," if trial it is, appears grossly unqualified to be running a clinical trial on something as tricky as testing whether stem cells might help stroke victims. If you don't believe me, take a look at Dr. Clemente Humberto Gil Zúñiga's CV posted on the Novastem website. He's a geriatrician who practices at Hospital Angeles Tijuana and appears to possess no relevant clinical trial experience that I can find listed. Certainly his publication record shows nothing related to stem cell biology or clinical trials.
I'm a clinical trial maven. That's why I had hoped to learn a bit more about the trial design, but the press release, not surprisingly, reveals little. Still, there are clues here. First off, this trial is designed to examine the effect of this stem cell treatment on aphasia. Briefly, the general term "aphasia" describes acquired speech/language difficulties due to brain injury or damage in which part or all of speech is impaired with no effect on intelligence. For example, in simple terms a patient with expressive aphasia can understand what others say and knows what he wants to say but just can't say it. I have personally witnessed a family member with this after a stroke. It's incredibly frustrating to the patient. There are other forms of aphasia, such as receptive aphasia, but it's not important for purposes of this post to describe them now. All you need to know is that various forms of aphasia are very common sequelae of strokes. It struck me as odd that Gordie Howe would be on an aphasia trial, because (1) his post-stroke impairments go way beyond aphasia, judging from the news reports and (2) he suffers from significant dementia, which would make determining aphasia scores difficult. We don't know for sure how bad Howe's dementia is, but in some news reports I've seen it's been described as "severe."
Next, there is this part of the title of the protocol, "Internal Research Protocol." Right away this tells us that there is no external funding; it's an internal protocol. Next, if we look at the paragraph above, we see a curious sentence stating that the "protocol is approved by the Research Ethics Committee of Clinica Santa Clarita, which is federally registered and licensed by the Federal Commission for the Protection against Sanitary Risk (COFEPRIS), a division of Mexico's Ministry of Health." What does this mean? Not being familiar with Mexican law with respect to clinical trials, as I am with US law, I am struck by how this is described. In the US, we would say that a trial is IRB approved (Institutional Review Board), that there is an IND (investigational new drug) application, and that the trial is registered with the FDA, which presumably any company would do because trials being used as a basis for drug approval have to be registered with the FDA and conform to all the rules for clinical trials, including the Common Rule. In this press release, we see from the sentence structure that it is the clinic, Clinica Santa Clarita, that is "federally registered and licensed by the Federal Commission for the Protection against Sanitary Risk (COFEPRIS), a division of Mexico's Ministry of Health," not the trial. I suspected that this sort of registration is not the equivalent of what goes on in the US. Boy, was I correct, far more so than I thought! I'll explain in the last section, when I look at this trial in more detail. First, however, I want to address a news story published right after Christmas.
What really happened?
On December 26, a reporter who's interviewed me before, Bradley Fikes, published a news story about Gordie Howe in U-T San Diego entitled "Did stem cells really help Gordie Howe?" This is the first—and so far only—attempt by a mainstream media outlet that I've seen to cast a skeptical eye on the whole story as presented. In the story, Fikes reports a number of disturbing aspects of this case.
First, we learn from Dr. Murray Howe, Gordie's son, how he's doing:
Howe, 86, suffered the stroke in late October, leaving him unable to walk and disoriented. He began improving within hours after receiving the stem cells in early December, said Dr. Murray Howe, a radiologist and one of Howe’s sons. For example, Howe insisted on walking to the bathroom, which he previously could not do.
"If I did not witness my father's astonishing response, I would not have believed it myself," Murray Howe said by email Thursday. "Our father had one foot in the grave on December 1. He could not walk, and was barely able to talk or eat."
"Our father's progress continues," the email continued. "Today, Christmas, I spoke with him on FaceTime. I asked him what Santa brought him. He said 'A headache.' I told him I was flying down to see him in a week. He said, 'Thanks for the warning.'"
Yes, Gordie Howe did appear to have "one foot in the grave" on December 1, although by a few days later he was doing better. Fortunately, he was just dehydrated and rapidly improved with hydration, as several contemporaneous news stories reported before Howe was ever taken to Tijuana for Novastem's stem cell treatment.
In fairness, I have to acknowledge that there's more:
A physical therapist who works with the elder Howe, Deirdre Bailey, said Thursday he showed "marked improvement" when she saw him a few days after the stem cell therapy. Previously able to stand only with extensive help, Howe could stand and walk on his own, although unsteadily and in need of close watching.
Bob Jones, a speech language pathologist who has worked with Howe over the last several weeks, said Thursday that Howe greatly improved his understanding and response to questions after the treatment. He was further improved when seen on Thursday of last week.
"He interacts more than he had before," Jones said. "He responds appropriately to such things as proverbs, idioms similes," when prompted to complete them. His speech, almost unintelligible before, is less difficult to understand.
So it does sound as though Gordie Howe is doing better, which is great. However, it's not possible to tell whether this improvement is due to his stem cell infusions. Remember, just before he went to Tijuana, he had recently been hospitalized for dehydration that had rendered him unresponsive. Before that, he had had a rough November, with setbacks but overall small improvement. Indeed, if you look at the news coverage of Howe's condition since October 26, you'll see reports of rapid recovery mixed with reports of setbacks. It's clearly been a bit of a rollercoaster ride, which makes it very hard to tell if any improvement is due to anything other than the nature the stroke, or if it's durable. The point is simple: Given Howe's fluctuating, but overall slowly-improving condition, it's hard to attribute his current condition to the stem cell treatment.
As hard as it is for Dr. Murray Howe to realize, as well, human beings are very prone to observational quirks. In fact, it's clear that he doesn't recognize it, given that the story reprints a complete e-mail by him in which he declares himself "an expert in my dad's medical condition" and "confident that my credentials attest to my capacity to be a reliable witness." (He also stated emphatically that he had written the entire December 19 press release announcing Howe's "miraculous" progress since undergoing stem cell treatment.) Unfortunately, doctors are arguably among the worst when it comes to overestimating our capacities to be reliable witnesses. Unlike our unfortunately-frequent view of ourselves as being objective observers, unless we make a conscious, skeptical effort not to be, we are just as prone to confirmation bias, in which observations that agree with our beliefs or hopes are more likely to be remembered and those that do not tend to be forgotten, as anyone else. Like every other human, we confuse correlation with causation.
In fact, if there's one thing I learned from watching my mother-in-law slowly die of breast cancer six years ago, it's that being a doctor does not inoculate one from hanging on every observation hopefully, latching hopefully onto anything that seems like an improvement, even if ephemeral or not even real, and discounting anything that looks like a turn for the worse. And that was observing a disease that is my specialty. Dr. Howe is a radiologist; he's not a neurologist or stroke expert. Let's just put it this way: Emotional connection plus confirmation bias do not equal a witness any more reliable than average. There's a reason why doctors generally do not treat loved ones. Emotional attachment affects judgment a lot more than we would like to admit. Emotional attachment also makes one prone to denial. I know this from personal experience too. Indeed, I could give you a specific example from when my mother-in-law's cancer recurred in which denial led me to a very stupid conclusion about a finding, but I'm too embarrassed about it to admit the details to any but my closest family.
But let's say that Howe really is as much improved as has been described, which, again, would be awesome. That still doesn't really mean that it must have been the stem cells that were responsible, given that he had recently been hospitalized and had had a rocky course. Certainly everyone seems to be assuming that it was the stem cells. For instance, the physical therapist saw him "a few days after" the treatment. When did she see him last before that? When he was in bad shape at the end of November and in early December? The same question applies to the speech therapist. Again, correlation does not necessarily equal causation. For example, on December 3, the Detroit Free Press reported:
Son Mark Howe told the Free Press that Gordie Howe has had a hard time sleeping since being hospitalized Monday. "Anxiety from dementia does that to him," Mark Howe wrote via text. "Change of surrounding makes his dementia worse as well."
With this in mind, it's hard for me not to ask: How much of Howe's apparent improvement was due to his having been home a few days after a hospitalization from December 1 to 3 that was followed by a trip to Mexico a few days later, and how much was due to the stem cell treatment? It's really not possible to say, but news accounts before Fikes' sure gave the impression that it just had to be the stem cells. Clearly Howe's family believes that. It's also rather difficult, even if one accepts stem cells as a promising treatment, to believe that stem cells fixed Howe's speech and motor centers so rapidly. It would seem likely that it would take longer than a day or two for such a dramatic recovery to manifest itself.
Stemedica and Novastem's responses: Not reassuring
After Fikes' story broke, I knew, in light of Stemedica and Novastem's joint press release, that I had to update the story. Being a clinical trial guy, I was frustrated, however, that what I really wanted to know was not in either Dr. Howe's press release, Novastem and Stemedica's joint press release, or Mr. Fikes' story. Here's what I wanted to know:
- The protocol (or at least the schema for the protocol) for the Novastem stroke trial (or contact info for someone who could provide me this information), including: (a) the full list of inclusion and exclusion criteria for the trial; (b) the full list of primary and secondary endpoints being assessed in the trial; (c) the date of IRB review and final approval by Mexico’s regulatory equivalent of the FDA; and (d) any preclinical data supporting the trial that has been published in the peer-reviewed scientific literature.
- Why is the Novastem trial not registered with ClinicalTrials.gov or Mexico’s COFEPRIS registry, as I mentioned above?
- Do subjects in the Novastem trial pay for their treatment?
Regarding the last question, I was particularly curious about this issue in light of Novastem's policies of cash on the barrelhead for treating basically anybody, as clearly delineated on its website, the statement in Fikes' article that patients pay for this trial, and this statement from Dr. Howe:
Did Novastem treat our father for free? You betcha. They were thrilled and honored to treat a legend. Would you charge Gordie Howe for treating him? None of his doctors ever do. I certainly am not going to criticize them for being generous.
I find it fascinating that anyone would criticize Novastem for charging, or for not charging, for their services. They appear to have developed techniques and protocols which are safe and hold promise for countless individuals. My hat is off to them for the quality service they offer.
As sympathetic as I am to the Howe family, I'm sorry, but I reluctantly have to say that Murray Howe really should know better than this. If Gordie Howe was treated as part of a clinical trial, then Novastem should have treated him for free because if it is running a clinical trial it should treat everyone on the trial for free. That's the way it's done ethically. I realize that these stem cell treatments cost something like $20,000 to $30,000 a pop, but pharmaceutical companies testing new cancer drugs, for instance, not infrequently spend way more than that per patient on clinical trials. It's the cost of drug development. Charging patients is also one of the big issues I've always had with Stanislaw Burzynski, for instance, charging patients to be on his clinical trials and justifying it by saying he's not charging them for the experimental drug (antineoplastons) but rather a "case management fee." In fact, I would argue that it's even more unethical if a company doing a clinical trial charges some patients for the trial but doesn't charge others, particularly if the reason it doesn't charge a patient like Gordie Howe is because he is a sports celebrity. What about all the rest of the peons who aren't famous? According to Fikes' story, they get charged $20,000.
In trying to answer other questions, through a circuitous route I found myself in e-mail contact with Dr. Maynard Howe (no relation to Gordie Howe), the CEO of Stemedica. He was pleasant and more than eager to talk to me about Stemedica's products, but, after some back-and-forth by e-mail, it became apparent to me that he couldn't (or wouldn't) provide me with any useful information about the Novastem clinical trial that I craved. Even though it had been he and Dave McGuigan, VP of Stemedica, who had reached out to the Howe family and facilitated Gordie Howe's treatment in Tijuana, my impression was that he was basically washing his hands of the matter, referring me to Novastem for all questions because it wasn't Stemedica's trial. So I tried the Novastem general contact page and, ultimately, the e-mail address for the PI of this trial, Dr. Clemente Humberto Zuniga Gil, listed on his CV page on the Novastem website. I don't know whether it was my e-mail through the general contact page, my direct e-mail to Dr. Gil, or, again in fairness, my previous communication with Maynard Howe having led him to contact Novastem that provoked a response, but on Saturday afternoon I received an e-mail response from the president of Novastem, Rafael Carrillo.
Mr. Carrillo was pleasant and accommodating. His e-mail responses struck me as very earnest and eager to explain his company's position, stating that he was looking into registering Novastem's clinical trial with ClinicalTrials.gov and COFEPRIS. He even sent me a PDF file containing a rather bare-bones clinical trial schema and tried to educate me about Mexican regulations governing clinical trials. Unfortunately, the information he gave me confirmed some of my misgivings about the trial and created others. For example, remember when I expressed puzzlement earlier in this post about what the clinic being registered with COFEPRIS meant? Well, he informed me that it meant:
As it states in our press release Clinica Santa Clarita is federally licensed to administer stem cell therapy. This means that the Mexican regulatory agency has authorized Clinica Santa Clarita and its doctors to apply stem cell therapy as the doctor sees fit. With the abundance of research across the globe and with the safety profile and high level of manufacturing Stemedica utilizes the Mexican authorities have felt it is justified to grant us a license to administer, as well as importing and banking stem cells. We treat all patients under IRB approved clinical trial protocols. We do this for two reasons, 1. We want to publish all our results. We want to share information. We believe that the more structured our data the easier it will be to publish. 2. We want to protect the patient. We have inclusion/exclusion criteria, informed consent, adverse event reporting, etc. At this point not everyone is a candidate for treatment. We want to make sure we are ethical in selecting patients for treatment.
So, in other words, the "federally licensed" part that confused me means that Clinica Santa Clarita can do pretty much anything it wants with stem cells, which is no doubt how it has been able to advertise its services and treat patients off-protocol in Tijuana. Learning this actually opened my eyes greatly as to how a weak regulatory environment in Mexico allows all sorts of dubious stem cell clinics to thrive there. In fairness, it is to Mr. Carrillo's credit that he wants to do clinical trials and ultimately publish his company's results. However, there is a problem—several, actually. First among them, as I pointed out before, the doctors with whom he is working appear not to have the requisite background in clinical trial design or stem cell science to produce a clinical trial that will generate useful data (more on that in a moment, when I discuss the clinical trial itself). He needs experienced clinical trialists, and I just don't see any. Another problem is that he doesn't seem to realize that in order to publish his clinical trial results in a decent journal, particularly one that follows the ICMJE guidelines, he had to have registered the trial with ClinicalTrials.gov or COFEPRIS before accruing patients. It's too late now; Novastem's already accrued one patient.
More problematic from an ethical standpoint is that Novastem charges patients to participate in its trials. In his e-mail, Mr. Carrillo tried to justify why Novastem charges patients for clinical trials:
Another issue you have brought up is payment. We are participating in patient funded research. We feel patient funded research is a viable option for both patients and doctors alike. On one hand we are not a billion dollar corporation that can fund all research, on the other hand we are following the examples of institutions such as the Mayo Clinic and MD Anderson Clinic who use this model. Patients know they have to pay. No promises are made to patients. It is very clear to all involved. We, and the IRB, feel there is enough evidence of safety and efficacy in the journals and doctor experience to proceed. Patients who choose to participate with us feel the same way. At no point do we hide this point.
In this particular trial the cost is around $30,000. Over half the cost is the cells alone, in addition to that we pay for the follow up work, the cost of patient recruitment, doctors fees, facility use fees, etc. Although $30,000 is a lot of money, to put it in perspective, it is also the cost of a knee replacement. Without being an expert in the field I believe that if this therapy proves to be effective, the cost benefit analysis will prove that getting the treatment is a good option. Also, like everything else that is new, with time and economies of scale price will go down substantially.
It was at this point that I heard disturbing echoes of Stanislaw Burzynski and his justification for charging patients tens—or even hundreds—of thousands of dollars to be on his clinical trials. It's also a misunderstanding of how cancer centers like M.D. Anderson do things. For example, the M.D. Anderson website specifically addresses this issue, stating that "if you are participating in a clinical trial, the trial sponsor, embassy or your insurance company may cover some of the charges. Items paid by the clinical trial will be listed in your Charge Estimate Letter" and that "you or your insurance will be responsible for the charges not covered." Generally, sponsors of the clinical trial have to cover the cost of the drug (or, in this case, biologic) and care that's normally not part of standard of care but is related to the trial (such as additional scans or tests). Presumably, that's how Stemedica's trials work north of the border. Admittedly, this method leaves a big hole. Patients who don't have health insurance will often have a huge difficulty paying for their care not related to the clinical trial and thus will have difficulties accessing cutting-edge clinical trials because they can't pay for their own regular care. Yay, USA!
What about the clinical trial?
First, according to the document supplied to me, this trial underwent IRB approval on September 28. It is summarized thusly:
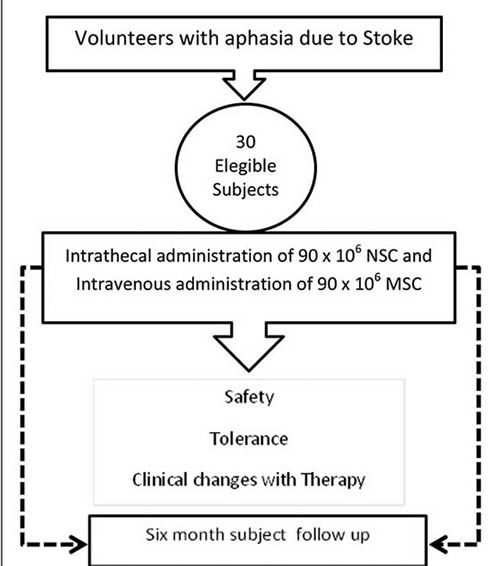
This is a pilot study in which a group of 30 volunteer subjects, with motor aphasia due to stroke will receive 90 x 106 of NSC intrathecally and an intravenous infusion of 90 x 106 of MSC. Leaving a window of 24 hours in between therapies. The subject follow up will continue for six months to verify safety, tolerance and to evaluate preliminary efficacy over speech, neurological function and quality of life.
This is roughly the same number of stem cells used in the Stemedica trial (one million per kg), but given intrathecal (into the cerebrospinal fluid) and intravenously. Here is a diagram of the study:
It's a fairly basic design, with these inclusion criteria:
- Age 45 years or older
- Motor aphasia based on the neuropsychological evaluation.
- Evidence of ischemic lesion on MRI.
- Capacity to understand and sign the informed consent based on the neuropsychological evaluation.
- Commitment to continue with medical evaluations and follow up.
- Adequate functioning of diverse organs defined by a number of common laboratory values.
Regarding #4, it is known that Gordie Howe suffers from significant dementia. It is thus highly unlikely that he was able to understand and sign the informed consent, but I suppose I could be wrong about this, given that I don't know the result of his neuropsychiatric evaluation. There's no mention that the family can give consent for the patient; so I assume that, strictly following the protocol, they can't. In fact, the exclusion criteria are:
- Global aphasia based on neuropsychological evaluation.
- Cognitive deterioration based on neuropsychological evaluation.
- History of cancer during the past 5 years.
- Subjects with oral steroids.
- Positive or reactive to HBV, HCV, VDRL or HIV.
- IMC ≥ 35.
- Pregnant women.
- Psychiatric abnormalities or abnormalities in the analysis based on the investigators criteria that might jeopardize the patient safety.
- History of alcohol or drug abuse and/ or smoking.
- Blood thinners seven days prior to the therapy.
This study is a not-unreasonable phase I study, albeit not particularly well designed. For one thing, it lacks a dose escalation component, in which doses are ramped up in order to estimate the maximum safe and tolerated dose, and some important inclusion criteria (more later). Also, its endpoints aren't well described and, as designed, highly unlikely to detect any statistically-significant evidence of neurologic improvement, given that there is not a strong attempt to make the group being tested more homogeneous by, for instance, setting limits on various scores. I also wonder how Novastem defines the ability to understand and sign the informed consent. There's also the issue of how cognitive deterioration is defined. Given the news reports, it could well be that Howe's cognition was deteriorating, but, equally importantly, it could well be that he was getting a bit better. That's where the Stemedica trial is actually better. It includes criteria requiring neurologic stability; without that, so soon after a stroke, it's almost impossible to tell if improvement is likely due to the treatment or if it's just improvement that was occurring as a normal part of recovery.
There's another issue. In Fikes' story, Dr. Murray Howe gives the following rationale for wanting to get his father on the Novastem trial ASAP, based on his having "one foot in the grave":
However, the [Stemedica] trial requires participants to have had the stroke at least six months ago. So Howe wouldn't qualify until late May.
Even more to the point, there was substantial doubt whether the elder Howe would survive for six months, or even until Christmas, said Murray Howe. Howe enjoys physical activity, and if unable to move he would lose his will to live.
I totally understand the Howe family's desire to throw a "hail Mary" pass to try to save their dad (or at least make him more functional and improve his quality of life). My wife and I looked for the same thing when her mother was dying from metastatic breast cancer, which is why we had her evaluated by the phase I group at my cancer center. I've been on both sides. However, in designing and carrying out a clinical trial it's critical to be very careful not to feed into the normal desires of family to do something. It's equally important to remember that, no matter how much you repeat that "there are no guarantees" or that "this probably won't work," the family will latch on to the chance that it will work. That's part of the reason why "patient-funded" clinical trials, as Mr. Carrillo describes them, are inherently prone to becoming exploitative. Just look at Stanislaw Burzynski, if you don't believe me.
If Gordie Howe really was deteriorating so rapidly four weeks ago that there was substantial doubt about whether he would survive until the end of the year, then he probably should not have been a candidate for any clinical trial for stroke. Indeed, most clinical trials for chronic conditions like stroke (and even cancer) exclude patients who are deteriorating so rapidly because they are incredibly unlikely to benefit and they make it hard to detect a real benefit if there is one. Indeed, notice how the Stemedica trial has an inclusion criteria of "life expectancy greater than 12 months." In marked contrast, there is no equivalent inclusion criterion in the Novastem trial, which is a huge gap.
Finally, the Novastem clinical trial is designed to examine the effects of stem cells on aphasia. A man who suffers from, if news reports are to be believed, significant dementia and, if Murray Howe's account of his father's condition in early December is accurate (and I have no reason to doubt it), Gordie Howe truly had "one foot in the grave" to the point where his son Murray didn't think he could wait "even 30 days for a Compassionate IND treatment in the United States," then he was not a good candidate for a clinical trial—any clinical trial, although an expanded use IND might still have been appropriate, particularly given that reports in early December from Howe's other son Mark described him as "doing better overall than he was several weeks ago when he had a massive stroke" and that he had "improved enough in the past 24 hours to where we expect him to be out of the hospital and in his own bed at home before the night is over."
Hope vs science vs exploitation
In clinical trials of new therapies, particularly for conditions that are either currently irreversible and result in a greatly diminished quality of life (like a stroke) or that will ultimately kill the patient (like certain cancers), it is always difficult to balance rigorous science versus hope and wanting to help as many patients as possible. After all, hope is part of why such patients enroll in clinical trials; that cannot be denied, and good clinical trialists are acutely aware of this. However, the ethical researcher tempers that hope and tries to keep it from being unrealistic. Moreover, as the example of my own experience with my mother-in-law's stage IV breast cancer and the writings of Dr. Murray Howe about his father show, being a physician does not inoculate one from unrealistic hope and human cognitive shortcomings like confirmation bias. As physicians, we find this hard to admit to ourselves, but it's true.
Similarly, it is potentially exploitative to require patients to pay to be on a clinical trial. That's why legitimate trials in the US don't require it, except in very uncommon, highly defined situations, and even then it is generally frowned upon. It is also highly unethical to treat patients on clinical trials differently based on their status. Ideally, none should pay to be on a trial, but if patients are being made to pay then it is, in my opinion, breathtakingly unethical to excuse one patient from paying just because he is a famous sports icon. It's more unethical when that patient is used for publicity, as Gordie Howe has been. Such a special financial arrangement is inherently unfair to other subjects on the trial. Worse, it also smacks of paying a clinical trial subject for an endorsement and is thus potentially coercive. It is profoundly disappointing to me that neither Mr. Carrillo, Dr. Maynard Howe, nor Dr. Murray Howe appears to grasp this. Indeed, Murray Howe dismisses such concerns by writing that there were "no strings attached to [Stemedica and Novastem's] offer" and that they "never have asked us to share Mr. Hockey's amazing response." Assuming that's so, unfortunately the lack of explicit "strings attached" or explicit requests to publicly share Howe's response don't make the arrangement any less unethical or potentially coercive. Indeed, Howe points out that he shared his father's response out of a sense of obligation, which is exactly what such arrangements engender and why they are unethical!
The saga of Gordie Howe's stroke and his treatment at Novastem is a textbook example of why clinics like Clinica Santa Clarita are a major problem. Accountability is minimal to zero, and patients pay for experimental treatments. Unlike the case with Dr. Burzynski, I actually think that the leadership of Stemedica and Novastem believes in the Stemedica stem cell treatment. However, it is very difficult now, knowing what I know, not to walk away with the impression that Novastem was a tempting way for Stemedica to sidestep the regulations of the US and that Stemedica, its leadership apparently believing in a stem cell miracle, yielded to that temptation. Meanwhile, Mr. Carrillo seems to want to do the right thing but appears not to understand what the right thing is—or to have any clinical trialists working for him who can tell him what the right thing is.
Perhaps the saddest thing to me is that Dr. Murray Howe feels sorry for "anyone who finds this miracle 'troubling.'" Presumably he means skeptics like Dr. Knoepfler and myself who have publicly questioned the news reports. I can assure Dr. Howe that I do not find Mr. Hockey's progress and recovery "troubling." No one, least of all myself, begrudges the Howe family hope. Indeed, I really do hope that Howe is doing better. I even hope it was the stem cells! After all, I'm not as young as I used to be. Cardiovascular disease runs in my family. I could easily find myself in Howe's situation 20 or 30 years from now. I would love it if there was an effective treatment for brain damage due to stroke, and I do believe that stem cells have great potential to treat conditions that were previously untreatable.
Unfortunately, it's everything else about his story that I find troubling, particularly how it was announced in the media, leading to numerous credulous reports portraying Stemedica's stem cell treatments as some sort of miracle cure for Mr. Hockey and how Howe's story as related by his family came across as very much of a piece with alternative medicine cancer cures and cures for other conditions. There is a right way and a wrong way to test treatments like this. Novastem looks as though it is taking the wrong way, whatever the motives of its president. Stemedica, too, is doing it the wrong way by trying to have it both ways, running legitimate clinical trials in the US while selling its product to be used however Novastem and Clinica Santa Clarita see fit. I feel obligated to point these things out not because I find Mr. Hockey's reported recovery "troubling" but because not every stroke patient is Gordie Howe.
Agreed that Murray Howe, even if he were an expert on the subject, should not be considered a reliable observer. He is, as they say, an interested party. There is nothing wrong with hoping, but hope is not always reality.
I was aware that Mexico has a reputation for hosting dodgy medical clinics offering dubious treatments to cash-paying customers, but it seems they have a huge hole in their regulatory structure--what they have is in some ways worse than no regulation at all, since in the latter case "caveat emptor" would be a given. It's not that there are no honest scientists (I have met a few, but they are in geophysics, not medicine) and doctors in Mexico, it's simply easier to be dishonest, at least in biomedical fields.
Orac,
Thank you for such an in-depth and thoughtful analysis. I don't always agree with your views but, boy, do you make me work to differ. :-)
Your blog is a public service.
tom
This is an excellent article and I am loath to interrupt the thread
even tho' it is Friday during a prolonged holiday and late HOWEVER-
I do sincerely apologise in advance ...I really do. Honestly.
OT but are new year's announcements by woo-meisters who would blithely capitalise on normal fears about the future ever TRULY OT @ RI?
Mikey declares 2015 the 'Year of Self-Reliance'** wherein we learn that all systems upon which we rely are **CRUMBLING**
food... water...finance.. medicine...community safety..power
are all on their way out.
Big Government/ the Nanny State/ the Police State will soon take loot your bank account and decimate your pensions whilst they lie about inflation, unemployment and GDP figures..
You need to become self-reliant, living sustainably and in harmony with the land
Go to farmers' markets, barter don't buy, collect rainwater, learn how to defend yourself with a gun. grow food, preserve and can your crops, raise chickens, get off the grid, go solar, home school, go to NDs, grow herbal medicine, try open source software, use a wood stove to heat...
Let's all go back to the 19th century, says Mike, and "I'll show you how!" via 3D printers!
( similar material @ PRN- sans the printers= where Gerald Celente declares a financial crisis will occur soon: BUY GOLD!!!!)
** and self-servicing?
Hey, now. Open source software is the sh*t. :)
I have aphasia, due to my two strokes. Thank you.
This is wrong and anybody who sees it knows it is wrong, and, yes, it is incredibly frustrating to be me (or someone like me) NOW, because I can understand,you goofs... I can't respond like I used to... But I am aware of it, and it's VERY frustrating.
Thank you for your clear explanation of what that, aphasia, means. I learn a lot reading here.
Comrade Carter--
how quickly are you able to respond by written format, i.e. your comment here?
Have you found that the heuristic typing methods speed it up for you--it's the type of texting that anticipates what words you are typing, so you don't have to cycle through each letter individually to get the ones you want when you use alphanumeric keys? I think there's a different version for keypad phones and touch screens but not sure what they're called--on my phone it's called T9Word.
Denice @ #3:
There goes Mike Adams again. Shouldn't he quit while he's ahead on his doomsday predictions?
Suppose society were to collapse in the manner that he predicts. Would being self-reliant in the ways Adams mentions help one in this case? If not, then who would be the most likely people to survive such a societal collapse?
I read this blog and your not-so-secret blog every night before bed. These posts about research methods and ethics are my favorites. Thanks for the great reading material.
@ Lucario:
Actually, you can read how accurate his 2013 predictions were ( see rational wiki/ natural news/ 2013 predictions)...
In short, not very.
He, Null and Celente ( see Trends Research) portray themselves as being incredibly perceptive and having insider information thus they can see into the future clearly. It must be a mark of their innate brilliance and purity of spirit. Or so they tell us.
Basically they play to fears: economic, health-centred and socio-political and then show a way out- by following them.
We came through a severe recession over the past few years, it makes sense that that trope would be frightening to most people. Everyone fears physical illness, death and harm coming to their family.
It's interesting that these guys preach 'crime and gang war' to those who live in cities ( esp NYC) when in reality, violent crime is lower than it has been in decades.
I feel that there's an underlying chord resounding whenever the words 'gang" and 'cities' are uttered and unfortunately, it involves distrust of minorities altho' they would confess that they haven't a racist bone in their bodies.
All three imagine a return to an edenic country-side, free of city vices and modernity: the 19th century farm village is the ideal -except for the internet of course. They assume that in a more static social order, great minds and spirits like their own, dripping wisdom, would naturally rise to the highest echelons of society like cream -even if they are vegans.
To be perfectly honest, I wouldn't be at all surprised if their average audience member is at least their intellectual equal.
They're talking to people who mistrust the world and using that discomfort to manipulate audiences into following them.
OBVIOUSLY they often warn their followers of 'liars and thieves' out to bilk them.
I have been suffering severe Thalamic pain ( also known as CPS and PSPS) since July, 2007, after two right hemisphere clot strokes in March, 2007. I was looking for help to alleviate my growingly sever left side pain when I first came upon stem cell therapy available at the Modern Cancer Hospital of Guangzhou, China. When they could not confirm that they had successfully treated a patient with my CPS, and after doubt was expressed by my doctors at Kaiser, I decided not to undergo the treatment in China. I then discovered, online, that a company in the U.S., StemGenex, was offering stem cell treatment for stroke patients, with treatment available in LaJolla and Santa Monica. After a few weeks of communication with StemGenex, and after paying $2500 "advance" against a fee of $15,000, I cancelled the procedure when StemGenex could not, or would not, confirm that they had successfully treated a patient suffering from CPS. After first contending that my $2500 deposit was non refundable, it finally relented and advised that my deposit would be returned (waiting anxiously.) friends shared the Gordie Howe news with me as an encouragement but now, thanks to your informative blog, I am resolute to deal with my pain as well as I can, while continuing to hope for legitimate clinical trials or other breakthrough leading to reliable CPS treatment. If any clinical trials surface, I am willing to be first in line. Thanks for your blog! :)
Denice @ #9:
That didn't answer my question. What I did ask was: Suppose society were to collapse. Would following Mike Adams' advice help in case of a societal collapse, and if not, who would be the type of person most likely to survive in the case of an actual collapse of modern society?
@Lucario - good question. The premise of the novel "The Postman" was that it was the survivalists that contributed to the ultimate downfall of civilization - since they immediately attacked and eliminated anyone and everyone who attempted to rebuild civil society.
@ Lucario:
I have no idea.
If you ever have viewed films like ' The Road' or 'Hunger Games,'** the survivors would be those with athletic skills, cognitive flexibility, practical skills/ knowledge and the ability to understand others' motivation.
If I were to write a novel about the collapse of modern society, I don't think I would follow the same formula as that.
And I don't suppose that being an Ardent follower of a braggadocious
fantasist like Mike would be helpful.
** I only saw parts of those films on television altho' I read 'The Road' ; I don't follow the zombie shows.
On second thought, I do know people who are descended from those who suffered devastation in early 20th century Armenia and whilst I only know a few, they seem to stress a strong cultural identity, powerful family ties and all speak several languages ( like Armenian, Arabic, Turkish, French, English). They learn how to fit into other societies where they are minorities- I imagine a certain of social flexibility is necessary. I know this is an exceedingly small sample.
Lucario--I thought the Hunger Games was a very important series to read. But it's science fiction in that several of the key weapons and medical treatments are far beyond current technological constraints.
Oddly, it was over at SBM that I obtained the name of a book I had read in the early 80s and forgot the title, which I can recommend you consider. It's quite dated in terms of the mores and societal structure (women's rights etc) but it's still an intriguing look at a post-apocalyptic world (a comet tail collides with earth). I wouldn't call it literature at all. The writing style is competent and interesting but it's realistic fiction and rather matter-of-fact in its tone if somewhat stereotypical; the interpersonal scenarios can get a bit silly at times but overall I think it's a worthwhile read. Try it: Lucifer's Hammer, by Larry Piven and Jerry Pournelle, 1977. Goodreads has several discussions you might find of value.
It was a fun read for me because I had forgotten how much of it was set in or near my old stomping grounds of LA suburbs.To read it once as a teenager and then as a parent with a very different perspective was also interesting when I compare my takes on the book.
"Lucifer's Hammer" - fantastic book, though I thought the ending for a bit anticlimactic...
I continue to speculate:
consider cultures which have been conquered/ invaded many times over the ages- what allows survival when alien hostiles encroach upon a town or village and impose their own ways? There are a few places in Europe which have such a history - Orac and a few of his minions originate from at least two of them Oh guess.
I think Mike is enraptured by American pioneer history and mythology such as that promulgated by old stylee movies. He's in his late 40s, so I can imagine what type of films he saw and the fantasy system based upon them. -btw- he liked the Hunger Games original film.
One that that hasn't been addressed in the reports on Mr. Howe that I can see (please correct me if I missed something) is whether or not Mr. Howe has been getting speech therapy and physical therapy post stroke.
I worked briefly in a rehab hospital. The results stroke patients would get with speech therapy and PT were nothing short of amazing . . . and that was in 1998.
Isn't it also possible that at least some of Mr. Howe's improvements are attributable to ST and PT? It seems to me that's why he wouldn't be eligible for a stem cell study in the US: the six months with no improvement is to make sure any positive benefits aren't the results of other efforts.
Continuing the off topic thread on post apocalyptic survival:
My favorite, and the one that I think would come closest to predicting what would really happen, is Alas Babylon.
The premise is a thermonuclear war in the early 50's (this novel was written around 1956 I think); the protagonists live in Central Florida and are cut off from the rest of the country by the radiation in major cities like Tampa, Miami, and Jacksonville.
Initially there is a certain about of selfishness that goes into survival. And there is a devolution of civil order. The hero, a lawyer, Army Reserve officer and Korean War vet, organizes a militia but operates on established United States law (the President had declared martial law). The society rebuilds a democratic society.
Mike Adams promotion of survivalist (Doomsday Prepper) thinking suggests he is either unabashedly an opportunist (since I don't see that kind of catastrophe happening) or a closet fan of the Turner Diaries.
Maybe both. He certainly is an opportunist.
What a way to make a living.
I'm suggest "A Canticle for Leibowitz" as a reasonably plausible post-apocalyptic vision.
In a post-apocalypse situation (I'm not sure I want to live there) I suppose people who are willing to help their fellow men and create a new society are better of, than those who consider everyone as a threat, like those survilalists one sees on television, or those who consider Mike Adams as their new Messias.
An old friend of mine who has suffered from MS for 30 years is desperate for some improvement. She has turned to your old buddy Dr Julian Whitaker. He claims to be able to cure MS with autologous stem cells harvested from adipose tissue. I tried to dissuade her by linking to this site but she is a true believer. As far as I know his clinic in Newport Beach CA is treating her out of pocket. I doubt Dr Whitaker has performed any clinical trials either to back up his claims. She is upset with for doubting her and Dr Whitaker. Doubting her alternative medicine is like insulting ones religion, dog or mother. It is often taken as a personal attack when it was not meant to.
The Secretary of HEW, actually.
Getting increasingly OT, but... @Denice (#17):
A combination of things, really: let's take the example of Poland under the partition. For one thing, yeah, strong cultural identity made a big difference. Poland had a long and proud history, and at one point was the richest and perahps most powerful country in Europe. (When it was a part of the Polish-Lithuanian Commonwealth.)
Second, the full partition - when Poland was off the map - "only" lasted for 123 years. In the Austrian part of the partition, Polish cultural traditions, university education, etc., were essentially left untrammeled. Things were somewhat worse in the Russian part, and worst in the Prussian section.
Third, Romanticism was huge in the 19th century, during the whole of which Poland (as a nation) didn't exist. A lot of Polish cultural figures practically worshipped Poland, even if they lived in exile. (Chopin, for instance, actually had his heart removed from his body after his death in Paris and brought back to Poland to be interred. I'm not making this up.) So you had a very strong national consciousness, which was maybe all the stronger in a way because of the partition. For instance, in the Russian section, about every generation there was a basically suicidal military uprising against the Russians - the "Polish spirit" refused to give up, even when it would have been wiser to do so. (You can see the same thing during World War II, the Warsaw Uprising, for instance.)
Okay, OT history lesson over.
,who would be the type of person most likely to survive in the case of an actual collapse of modern society?
A very well-armed gynecologist.
Re. _Lucifer's Hammer_: Am I the only one who's noticed how bloody racist that book is?
Blond-haired, blue-eyed white people (classic Aryans) depicted as smart (the nuclear plant crew), black people depicted as animals (and cannibals as well), and in the end the hero saves the day by mixing up a batch of chemical weapons and using them against the marauding blacks.
Sorry folks, but that book should be forgotten and let die an ignominious death. There's plenty of other apocalyptic fiction out there for a good scare without an overdose of racism.
--
I should mention, I flew over the holidays, and in the seat next to me was a woman who was reading some of the outrageous quackadoodle stuff we frequently discuss in this blog.
One thing she was reading was a thick pamphlet or thin book with all the usual drivel about detoxification and colon cleansing, with an overt pitch to buy the magic potions from the 'doctor' who was the author.
Another was a book with the word 'bulletproof' in the title and similar drivel in it (minus the sales pitch for power-placebos) that I managed to ascertain was written by someone who described himself as a formerly obese & unhealthy Silicon Valley exec or entrepreneur.
I was highly tempted to take out my laptop, on which I had open a couple of Orac's columns from that week, and just plop it on my tray table where she would see it and hopefully read a bit. I was also highly tempted to say something along the lines of, 'looks as if the people we read are competitors,' and direct her to this blog.
But in the end I thought it better to say nothing and leave her in peace: it's not as if I could persuade someone that what they believe in is utter quackery, and any unpleasantness on aeroplanes is to be avoided. None the less, interesting to run into a full-fledged case of what we discuss around here.
Yes people really do read that stuff and believe it. But at least she wasn't coughing and sneezing all over the place.
OT , but may be of interest - cancer, more a matter of bad luck than life-style:
http://www.bbc.com/news/health-30641833
@ Lurker #27:
Yeah, I read Lucifer's Hammer at the time and was thoroughly disgusted. All of Larry Niven's (not "Piven" as brewandferment spells it at 15) and Jerry Pournelle's work, both separately and together, is pretty right-wing bullshit. (I think Pournelle is several times worse than Niven.)
It's forgivable in The Mote in God's Eye for example, because the background polity is an Empire, after all, but in Lucifer's Hammer or Footfall, which are set more or less in the here-and-now, it's impossibly grating.
Mote really did revolutionize the field, though, you gotta give them that. What puzzles me is that the Motie civilization should be the ultimate libertarian wet dream, and so lionized by them—instead they treat it as the horror show it is. Peculiar.
Re. _Lucifer’s Hammer_: Am I the only one who’s noticed how bloody racist that book is?
You are not.
#26 Lurker: You were absolutely right not to try arguing with the woo-lady. My two sisters are also deeply into New Age fairy stories and alt-med crap, and resent it bitterly when I point out the logical contradictions and absurdities of their beliefs. This has caused some big family rows.
I went to a presentation by either the author of "Bulletproof Executive" or an ardent follower of it. Complete jerk, and claimed that the diet "cured his Asperger's" because he hadn't been able to make eye contact with people before the diet and then he suddenly wanted to do the eye contact thing.
So of course my ex-friends in the host group started pressuring me to follow the Bulletproof Diet so I could be cured.
shay @ #25:
Why a gynecologist, exactly?
Because it is to be highly desirable to include that specialized skill in a false flag, post apocalyptic, nomadic, on-the-go and sometimes quite spontaneous yet seemingly still inappropriate erogenous existence --
Emergency repair and mantainence of the woman-box from the rare specialist with warm, sterile hands and an even more sterile personality (so as not to induce clan-destroying jealousy) is one of the most crucial aptitudes one may demonstrate in a time of lack of affordable birthing of babies and neonatal tutelage of already survival-problematic teens (ever seen them going to town just as your plane is crashing??).
Besides, The last-minute prepper who decided they could probably bug out while foregoing the overpriced, bulky, and heavy "light-weight, superholofil, self-erecting birthing shed" in favor of more seeds has more seeds. Some seed is more useful than others in an economy of barter.
Tim @ #33:
What does seed have to do with it? I thought seed was a male thing. (Er-hem.)
Just out of curiosity, were midwives important in times of historical societal collapse? (And now I have the "I don't know nothin' 'bout birthin' no babies!" quote from Gone With the Wind echoing in my head, thankyouverymuch!)
Sorry, this is off topic but brief. I'm asking here because I don't know where else to ask. I'm trying to find out more about what I think is a new dietary scam, low histamine diet. If anyone has skeptical resources for this, please contact me by email, so I don't derail the conversation any further.
camilla-personal@mindspring.com
Thanks.
Cripes, being a gynecologist/midwife/man-midwife during the breakdown of civilization would be a horrible career move!
Can anyone provide an example of a society or culture where they were high-status, rather than a joke (until the 20th century)? Hypothetic "goddess-cultures" don't count.
Perhaps I'm overly influenced by Margaret Atwood's "The Handmaid's Tale" but I could see a clique of powerful men controlling resources - weapons, food, gold whatever...take us back to the middle ages and the divine right of kings.
Ensuring that women survive childbirth? What for? chance to get a younger more compliant one!
But there seems to have been some SBM resistance, of late:
I should imagine that in this ongoing, er-hem, *collapse* that a burgeoning technocracy which freely passes around the epidurals and abortions over social interaction and pot would consider the rouge midwife somewhat of a "high-value target" (HVT) to be tracked down and summarily reeducated in the ways and by the ways of SBM.
I guess, right about now, that I'm picturing scenes from Children of Men set to the tune Strawberry Fields Forever:
https://www.youtube.com/watch?v=LZo1T7KOgs4
The Very Reverend Battlaxe of Knowledge
Unsurprisingly Jerry Pournelle is a vocal AGW denialist.
Mike Callahan
Is your friend aware that Whitaker is a Scientologist?
OT but are pseudoscientists, claiming to have new, simple technology that will SAVE THE WORLD, who need to announce that it doesn't quite work prior to its official internet release, EVER truly OT @ RI?**
And yes, Mikey never disappoints us:
his new invention created by Lulzbot (tm) is bolluxed up because of extrusion problems*** ( see Natural News today).
** I thought that this OT would neatly match my OT of Friday
*** and what isn't?
Lucario @ #32-- to identify the healthy breeding females, of course.
Going to butt into the doomsday scenario discussion to ask, does anyone have any idea of how long a stem cell treatment should take to show effects? The cells would need to settle, differentiate, and integrate into the damaged tissue, it seems like that would take more than a few days...