
A frequent topic of discussion on this blog is the concept of overdiagnosis. It’s a topic I’ve been writing about regularly since around 2007 or so and is defined as the detection in an asymptomatic person of disease that, if left alone, would never progress to endanger that person’s life or well-being within his or her lifetime. The problem with overdiagnosis is that it pretty much always leads to overtreatment, the treatment of overdiagnosed disease that is not health- or life-threatening. The key shortcoming in our knowledge that leads to overtreatment is that, once we detect disease with many screening tests, we usually do not have any tests that can identify which lesions are potentially dangerous and which ones can be safely watched because they are unlikely to progress (or to progress fast enough) to be a problem within the patient’s lifetime.
Most commonly, I’ve discussed overdiagnosis in the context of mammographic screening programs, but I’ve also looked at the overdiagnosis of thyroid cancer, prostate cancer, and other diseases. The bottom line, from my perspective, is that screening asymptomatic populations for breast and prostate cancer does have some benefit, but over the years that benefit was likely exaggerated as the downside of screening (overtreatment) underestimated. On the other hand, there are those out there whom I view as nihilists, who have gone too far in the other direction, declaring certain forms of screening (particularly mammography) to be worthless or even harmful.
The purpose of that preamble is to let new readers know where I’m coming from, as what I’ve just written will have been no surprise to regular readers. The longer you’ve been a reader, basically, the less of a surprise it will be. So you can probably predict how I reacted to an article that’s been going around social media since it was first published four days ago. In fact, I was going to write about it yesterday, but my Dug The Dog complex hit, and I was distracted by two articles in the latest New England Journal of Medicine. Still, many of you can guess which article I’m talking about, as the title is akin to my retort to an article by a fellow physician that, no, the New York Times did not kill your patient, only in the other direction. This time around, it’s not a physician, but rather an actor and comedian, Ben Stiller, who wrote about The Prostate Cancer Test That Saved My Life. My response is not quite as definitive as my response about the NYT. In response to Mr. Stiller, I can only respond: No, the prostate cancer test probably didn’t save your life, but we can’t know for sure.”
Stiller is clearly very intelligent. His essay is well written and well-argued and even includes a poignant description of his reaction to his diagnosis of prostate cancer:
I got diagnosed with prostate cancer Friday, June 13th, 2014. On September 17th of that year I got a test back telling me I was cancer free. The three months in between were a crazy roller coaster ride with which about 180,000 men a year in America can identify.
Right after I got the news, still trying to process the key words echoing dimly in my head (probability of survival–vival-vival-val…” “incontinence-nence-nence-ence…), I promptly got on my computer and Googled “Men who had prostate cancer.” I had no idea what to do and needed to see some proof this was not the end of the world.
John Kerry… Joe Torre… excellent, both still going strong. Mandy Patinkin… Robert DeNiro. They’re vital. OK great. Feeling relatively optimistic, I then of course had to do one more search, going dark and quickly tapping in “died of” in place of “had” in the search window.
If you’ve just been diagnosed with cancer, never do that search, people.
Pretty much any cancer patient can relate to Stiller’s story, particularly if the cancer is a common one, like prostate, for which there will likely be lots of news stories about celebrities bravely battling the disease. Here’s where Stiller goes wrong, but understandably so given the issues involved:
Taking the PSA test saved my life. Literally. That’s why I am writing this now. There has been a lot of controversy over the test in the last few years. Articles and op-eds on whether it is safe, studies that seem to be interpreted in many different ways, and debates about whether men should take it all. I am not offering a scientific point of view here, just a personal one, based on my experience. The bottom line for me: I was lucky enough to have a doctor who gave me what they call a “baseline” PSA test when I was about 46. I have no history of prostate cancer in my family and I am not in the high-risk group, being neither — to the best of my knowledge — of African or Scandinavian ancestry. I had no symptoms.
What I had — and I’m healthy today because of it — was a thoughtful internist who felt like I was around the age to start checking my PSA level, and discussed it with me.
If he had waited, as the American Cancer Society recommends, until I was 50, I would not have known I had a growing tumor until two years after I got treated. If he had followed the US Preventive Services Task Force guidelines, I would have never gotten tested at all, and not have known I had cancer until it was way too late to treat successfully.
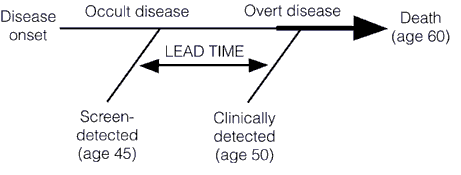
It’s understandable why Stiller feels this way and believes this. Also, in fairness, one aspect of Stiller’s case that tends to be in his favor is how young he is. Prostate cancer before the age of 50 is very uncommon. Be that as it may, it is a maddeningly intuitive notion that early detection always saves lives. Yet, as I’ve pointed out time and time again, beginning back in 2007, the relationship between the early detection of cancer and the likelihood of cure and long term survival is not nearly as straightforward as it seems on the surface. There are a number of factors that confound this seemingly obvious and intuitive relationship, but the two most important are lead time bias and length bias.
I’ll illustrate the concept of lead time bias with a graph that I’ve used many times before to explain:
And a slightly more complex one:

I have explained the concept of lead time bias in more depth here and here, but I do these graphs for illustrating the concept that lead time bias can make it look as though survival from a cancer screened for is longer even in the absence of any therapeutic effect whatsoever from treatment. Since it’s been a while since I’ve shown this particular graph, I’ll add it to the mix, as it shows the effect of lead time bias on cancer survival curves:

Before I move on, I’ll even cite Aaron Carroll again, as he gives one of the simplest and most straightforward explanations of lead time bias that I’ve yet to see. Of course, the phenomena of lead time bias and overdiagnosis are intertwined. Think of overdiagnosis as the detection of a tumor with a lead time, as illustrated above, that is longer than the remaining expected lifespan of the patient, and you’ll see what I mean (I hope). In such a case, patient survival will seem to be, in essence, infinity, at least with respect to the cancer in that the patient dies of something else before the tumor progresses significantly. Now, Stiller does make one good point when he says there might be high risk groups for whom PSA screening is appropriate, and there is certainly research looking at that very question. However, now, based on what we know now, for the vast majority of men at average risk for prostate cancer, PSA screening is more likely to cause harm through invasive testing and over treatment than to save their lives.
The other problem with screening tests that confounds the relationship between early detection and improved cancer survival is a phenomenon known as length bias. Basically, length bias is the term used to describe how regular screening tests tend to detect slower-growing, more indolent disease preferentially. How many of you know someone who had a mammogram on schedule as recommended but came back the next year with a big, advanced breast cancer. Did mammography fail? Probably not. Rather, the tumor was just too fast growing. It went from undetectable by the test (mammography) to advanced during the interval between screenings. More often, what is detected by screening tests like mammography is disease the grows relatively slowly. This concept is illustrated here, by another chart that I also like to use a lot:
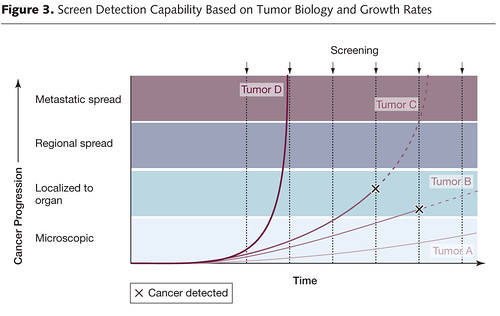
The other problem with length bias is that the more sensitive the test, the more likely it is to detect tiny indolent tumors that are so slow-growing that they wouldn't progress to the point where they would endanger the patient's life within the lifetime of the patient. Some, particularly screen-detected cancers, even spontaneously regress. Length bias and overdiagnosis are also related concepts in that length bias contributes to the tendency of screening tests to overdiagnose the disease they are looking for.
So, unfortunately, Ben Stiller is wrong in that there’s no way of knowing that the PSA test “saved” his life or that if he hadn’t been screened at all his tumor would not have been found until it was “too late.” Those are common assumptions on the part of patients and even many physicians. In brief, there is no surefire way of knowing whether or not he was overdiagnosed. However, as we’ve come to appreciate over the last decade, prostate cancer is very commonly overdiagnosed. In fairness, Stiller is definitely more savvy and informed than the average celebrity writing about medical issues. He clearly at least recognizes the controversies involved in screening:
The criticism of the test is that depending on how they interpret the data, doctors can send patients for further tests like the MRI and the more invasive biopsy, when not needed. Physicians can find low-risk cancers that are not life threatening, especially to older patients. In some cases, men with this type of cancer get “over-treatment” like radiation or surgery, resulting in side effects such as impotence or incontinence. Obviously this is not good; however it’s all in the purview of the doctor treating the patient.
This is exactly what happened to Stiller. His PSA rose for a year and a half before he was referred to a urologist, who did an examination and ordered an MRI. This led to a biopsy, which diagnosed a tumor with a Gleason score of 7 (3+4), which is categorized “mid-range aggressive cancer.” The Gleason score, however, is not the be-all and end-all as a criterion for starting treatment. Stiller doesn’t tell us how many cores of his biopsy contained cancer, whether cancer was found in both sides of the prostate, or how much of each core contained cancer, or how fast his PSA was rising. Be that as it may, he is far more likely than not to be mistaken when he declared so bluntly that the PSA test definitely saved his life. This infographic from the National Cancer Institute tells why there’s at least a 95% chance he was mistaken. In fact, for every 1,000 men who undergo PSA screening, only one life is saved, but 100-120 get false positive diagnoses and 110 will get a prostate cancer diagnosis. Again, it’s understandable why he would believe as he does, but that doesn’t make it any less misguided.
Let’s just put it this way. If even Dr. Mehmet Oz throws cold water on your claims, you should rethink:
Of course, Oz then went on to oversell dietary and exercise interventions for preventing death from prostate cancers, but you can’t expect Oz to do a whole segment without getting into some woo, now, can you?
The main problem with Stiller’s article, besides its mistaken argument that PSA screening almost certainly saved his life. He also cited a study by Edward Schaeffer, his surgeon and the chair of urology at Northwestern University, to support his point, stating, “There is growing evidence that these guidelines have led to increased cases of prostate cancers that get detected too late for the patient to survive the disease.”
You might remember this study, as it was in the news back in July. Basically, it purported to find that the incidence of metastatic prostate cancer has been climbing since PSA screening began to fall, the implication being that decreased screening is leading to more men being diagnosed with metastatic (and therefore incurable) prostate cancer. I first saw the study, but it was at a time when I had a lot of other things going on; so I didn’t look at it carefully. Concerned, I whipped off a quick e-mail to a relevant expert whom I trusted and had published with before asking him what he thought of the study and whether maybe I should consider starting PSA screening again. His response was blistering.
I’m not going to quote his e-mail directly because I do not publicly reveal e-mail contents without permission of the person who sent it to me. I can say that he did dismiss it, pointing out that, although the authors used the word “incidence,” what they were really counting were gross numbers of cases reported to the National Cancer Data Base (NCDB) from 1,000 health care facilities and changes in gross numbers from 2004 to 2013. He pointed out that true incidence is the number of cases divided by the number of people in the population (usually expressed per 100,000). So here’s the problem. Schaeffer’s group reported the numerator, but had no idea what the denominator was (the number of people in the population from whom the cases came from), as they even basically admitted:
Limitations to the current study include the lack of national annual incidence rates in the NCDB. Thus, our outcome variable was annual incidence of prostate cancer at over 1000 health-care facilities in the United States relative to that of 2004, the initial year of our study period.
In fact, the incidence of metastatic prostate cancer has been stable from 2004 to 2012 (the time period of the study cited by Stiller) and in fact the incidence was lower in 2012 than it was in 2000. Clearly, the incidence of metastatic prostate cancer is not increasing using more standard methods of measurement.
Suffice to say, I was horribly embarrassed for having asked about this study when in retrospect I knew enough to have figured out how useless it was myself.
Others have been critical of Stiller as well, for example, Kevin Lomangino, the managing editor of HealthNewsReview.org, who wrote Ben Stiller’s misguided prostate cancer recommendations aren’t based on evidence. He hit many of the same points I did, although he didn’t go into lead time bias and length bias, as I did and some I didn’t, noting, as I did, that Stiller is “smart, persuasive, and famous,” but that “his skewed piece may do a great deal of harm to men who may be led astray by his faulty reasoning.” He also cites oncologist Vinay Prasad, MD, MPH, who made a similar point to that which I’ve made many times regarding mammography:
Ben Stiller says everyone over 40 should get a PSA, but why does he discriminate against 39 year olds? If you accept Ben Stiller’s logic, that we should do anything to find cancer early (with near total disregard for net effects, harms or overdiagnosis), why is 40 Ben Stiller’s cutoff? He criticizes the American Cancer Society for 50, and yet equally arbitrarily chooses 40. If Ben Stiller thinks a 40 year old should be offered a PSA, why not a 39 year old? Why not every man? Since Ben Stiller does not employ careful scientific reasoning to reach his position, I would argue that Ben Stiller is logically inconsistent.
I’ve basically said the same thing about mammography to those criticizing newer recommendations that increased the age at which mammographic screening should begin for the average risk woman and argue for retaining the existing guidelines that recommend beginning at age 40. Why not begin at age 35? Or 30? Or even 20? In other words, even the most enthusiastic advocates of screening realize that there is an age below which incidence of breast cancer is so low that the harms from screening far outweigh the potential benefits. It’s always a judgment call to set those cutoffs, and there is always harm from overtreatment whenever there is screening with a significant incidence of overdiagnosis. Balancing the risks and benefits is what is so difficult about constructing screening programs for common cancers like breast and prostate. I only wish that Ben Stiller had done more than acknowledge those risks in passing and avoided concrete declaratory statements like, “Taking the PSA test saved my life. Literally.” And: “I believe the best way to determine a course of action for the most treatable, yet deadly cancer, is to detect it early.”
Unfortunately, we’ve been learning that this is not always true. It’s complicated. I am gratified, though, that the reaction to Stiller’s article has been, unlike what would likely have been the case in the past, to take him to task for making assertions not supported by evidence. Unfortunately, Stiller’s celebrity will likely trump evidence.
We recently discussed exactly this issue on the Great Orange Satan, in the context of Rudy Giuliani using confusion of mean survival times to sneer at the communist National Health in Britain, and the concensus is that many Kossacks are Really Fucking Stupid about the interpretation of medical statistics - but that doesn't stop them from having belligerent and contemptuous opinions.
Here's my take on that common right wing talking point:
http://scienceblogs.com/insolence/2012/04/24/more-cancer-care-isnt-alwa…
Orac, didn't you co-author a paper saying that PSA screening implementation led to a dramatic drop in prostate cancer metastasis?
FWIW, this article is a nice counter-point to the USPSTF recommendations against screening for prostate cancer: http://annals.org/mobile/article.aspx?articleid=1166178
Rather than relying on anecdotal evidence like Stiller's story, it does a nice job of explaining the flaws in their reasoning, and it's not behind a pay-wall, which is always nice!
There isn't really any way of determining if a prostate tumor will turn out to be dangerous (I dont think even Gleason scores do this adequately) and no way of telling if the tumor has already metastasized. Both of these are big areas of research.
2 years after treatment is a little too soon to be sure that there won't be recurrence.
Though I actually don't know the stats of how often we see metastasis if the primary tumor is removed before any are detected. It's not the area of research I am familiar with.
Having Gleason 3+4 prostate cancer at age 48 seems pretty high risk to me. Simply an elevated PSA at that age is associated with an 8 fold higher risk of death from prostate cancer (http://jco.ascopubs.org/content/early/2016/06/09/JCO.2016.66.7527 and a couple of other studies)
Leaving such a cancer until it produces symptoms gives a high risk of it already having metastasised, which is incurable although slow.
Two problems with the NCI infographic:
- it only considers death within 10 years of PSA testing . Deaths go up after then
- we have treatments that will control metastatic prostate cancer for 3 or so years, but they are quite unpleasant - chemical castration to start with. That's not death but worth avoiding.
Small low risk prostate cancers are common (about 50% of diagnoses) and should not be treated, but larger and higher risk once can kill. Low-Intermediate risk ones like Ben Stiller's take 10-15 years to kill but they are still dangerous. Mine was the same Gleason score but by age 52 it had already grown into a 20cc tumor. Leaving it for another decade would not have been wise.
I think the best PSA testing recommendation is to test once in the mid 40's to see if you're in the high PSA = high risk group. If not, leave it until 50+. Statement 4 in this: http://www.bjuinternational.com/bjui-blog/the-melbourne-consensus-state…
I'm 6-years post surgery, and my most recent PSA was below detectable limits - two more years of remission before "cured."
I started screening at age 50 - and for ten years it was in the normal range. 3.5 or so. Then it rose to about 4.5 in one year. Hmmmmm.
Next year it was 5.5, and the year after, 7.8. That's when my primary physician referred me to a urologist.. Not once did my PCP note any nodules during my annual digital exam, but the urologist found several right away.
Biopsy found 12/12 positive, Gleason score 7 (4+3).
Upon resection, the diagnosis was Stage II (b): clear margins, no infiltration to the capsule, no lymph nodes involved. At that rate of increase, I was probably two years away from metastatic disease, Lupron, and (mostly ineffective) chemotherapy.
The problem is not with screening per se, but with the response to the data. I agree with Mr. Stiller that screening might well have saved his life - it seems to have saved mine.
fusilier
James 2:24
I think it is difficult to second guess Stiller's decision to be treated without seeing the pathology report. In the absence of a family history, it is likely that he had a minimal prostate cancer, but that is not a given. If he had a large tumor, then the decision to be treated at age 48 is probably the correct one. There is still no guarantee that the PSA saved his life.
The timeline that he gives suggests that he had radiation, not surgery, because the urologists like to wait 8-10 weeks after the biopsies before operating so that the area is completely healed, and you have to wait almost as long after the surgery to do that first PSA in order to get an accurate result. That is perhaps not the best choice for a 48 year old. The consequence of failing radiation is a salvage prostatectomy which carries with it a very high incidence of complete impotence and complete incontinence. In my mind, it would be better to have the surgery first and save the radiation for a potential relapse. That's what I did at age 49. I have to wonder whether he was getting the best advice.
I don't know if something got lost in translation but incidence is the number of new cases/population at risk.
I'm aware of that. Missed the new cases. It's usually per year, too.
I can't argue with that, but Stiller didn't give us that information, unfortunately, which is why I mentioned that we need more information than just his Gleason score, which is basically all he gave besides his diagnosis.
Yep. Lead time bias means that it probably didn't, but there's a small chance that it might have.
@ Michael Finfer, MD:
I truly hope that you're doing well now.
I am always leery of population based statistics applied to individual cases. If there is consensus that PSA screening may have saved his life - saying it did or it did not are just political interpretations of that reality.
The population based arguments always assume a certain cost that individual patients and their physicians may not want to assume. I see this as the cost of biological complexity rather than who has the best argument.
Worth repeating:
"The United States Preventive Services Task Force has analyzed the data from the PLCO, ERSPC, and other trials and estimated that, for every 1,000 men ages 55 to 69 years who are screened every 1 to 4 years for a decade (5):
0 to 1 death from prostate cancer would be avoided.
100 to 120 men would have a false-positive test result that leads to a biopsy, and about one-third of the men who get a biopsy would experience at least moderately bothersome symptoms from the biopsy.
110 men would be diagnosed with prostate cancer. About 50 of these men would have a complication from treatment, including erectile dysfunction in 29 men, urinary incontinence in 18 men, serious cardiovascular events in 2 men, deep vein thrombosis or pulmonary embolism in 1 man, and death due to the treatment in less than 1 man."
https://www.cancer.gov/types/prostate/psa-fact-sheet
So yes, we should listen to Ben Stiller talk about how PSA testing saved his life - if we also listen to 50 men talk about the devastating effects on their lives of prostate cancer treatment. Their "roller coaster ride" did not turn out so well.
Here's hoping we get good molecular testing going ASAP so we don't have to depend on crude measures like PSA levels, Gleason scoring and so on. In the short term, adopting age-specific PSA reference ranges (to avoid over-biopsy/treatment in older men) would help.
That is how the best evidence base is formed though. Of course there will always be outliers. If you have a better way, I would be interested in hearing that. There can't be a "consensus" without all of the information. And no one here is saying with absolute certainty that it did or didn't.
Only because you mentioned Dug the Dog, here is a little bit of coincidental fun. Talking Dug Dog
I'm reminded that I've never had one. Is the standard of care to start at age 50?
Now here's an interesting take on going the opposite direction: Active surveillance.
http://www.medpagetoday.com/hematologyoncology/prostatecancer/58880
Narad beat me to it. If a 48 yr old had a 2X swolen prostate, would it be prudent to start getting the test at 50? I've gotten confused on if a swollen prostate leads to/is associated with cancer or not.
Is there anything to this https://www.superbeta.com/ or is it just another case of 'one weird trick to invert your dick'..
"If you have a better way, I would be interested in hearing that"
A better way was just posted by Orac above. I have followed a number of patient with cancer diagnoses who have lived a long life with this approach. I am not an oncologist, but I am treating them for other problems and need to know their associated conditions.
I am also undoubtedly biased by knowing men 50 years of age or less who died of aggressive prostate cancer. I would like to know how these outliers get reflected in the screening statistics of the US Preventive Services Task Force. Stiller is currently 50 years old suggesting the Task Force data may not apply to him.
I would have to disagree. This doesn't work on a population basis (see comment #15 Dangerous Bacon). Again, applicable to outliers but the number needed to treat would far outweigh any benefits and increase the risk of side effects from biopsies etc.
RE: Lead time bias.
Consider that the earlier you first get tested for xyz (assuming you eventually do get tested at some point), the longer your survival time will be after your first test, regardless of whether you even look at the results of the test or not. It's magic!
First tested at birth for xxy, die on your 80th B-Day, survival time =80 years.
First tested for xyz the day before you turn 80 & die the next day, survival time= 1 day.
QED.
Please get your first test as early as possible. :)
Isn't a biopsy a greater chance to spread cancer, should it exist?
Davidp@7: I was just listening to a presentation on the current state of treatment (approved and clinical trial) for metastatic castration-resistant prostate cancer and the oncologist made an interesting comment that many patients who are described as MCR have never actually had their testosterone tested, so we don't actually know that the disease is castration resistant, or if more vigorous application of androgen deprivation (sounds better than 'chemical castration') would still be effective.
It might be an area for urologists/oncologists to consider.
@#15
Bacon, one of the subtle problems with the USPSTF recommendations is that urologists and oncologists are now doing a better job of uncoupling the side effects of treatment from screening and biopsy. Active surveillance is now a rapidly growing part of the management strategy for lower risks forms of prostate cancer. Using information from MRI and molecular testing, many patients can go for years without requiring treatment. Add that to the fact that PSA screening does save lives, according to the best studies done on the subject (i.e. NOT the PLCO trial), and a recommendation against screening seems foolish.
Read the best ever PSA screening medical journal article by a former Stanford Prof of Medical Ethics written in 1996!
http://ijme.in/index.php/ijme/article/view/1765/3803
These authors and other articles I've read would take issue with Orac's statement " Prostate cancer before the age of 50 is very uncommon." The articles cites autopsy studies of men who've died of unrelated causes showing 30% of men in their 40's with pathological evidence of cancer. Other autopsy studies I've read have shown pc in 8% of 20 year olds and increasing incidence all the way up to 100% of 100 year olds. The inventor of the PSA test has been quoted as saying that all you need is an excuse to biopsy and you'll find cancer. That is somewhat supported in this old article about a poor guy who's doctor inadvertently tested his blood for PSA as part of a routine physical when he was 29 years old: http://online.wsj.com/public/resources/documents/SB110350121947304355.h…
Methinks you're bordering on pedantry here. I thought it was clear from the context that I meant clinically evident prostate cancer requiring treatment. After all, over 75% of men over 80 have foci of prostate cancer in their prostates, but the vast majority of them die without clinically evident prostate cancer.
I've written about this very issue myself on more than one occasion, but you appear to be new; so it would be unreasonable for me to expect you to know that.
Well then I'll go on and take issue with your interpretation of "clinically evident requiring treatment." Just where are the studies and data to support the notion that Stiller's Gleason 7 (3+4) requires treatment? We do have a great study that shows that Gleason grade progression is uncommon. http://www.medscape.com/viewarticle/809443 “These findings suggest that grade may be established early in tumor pathogenesis,” conclude the authors
How do we know anyone truly has clinically evident pc requiring treatment? Have we ever randomized localized Gleason 7 patients into treatment and non-treatment groups?
Ok I'll check out your past posts. I wonder if you had ever seen the medical ethics journal article I referenced and what do you think of it?
As a non-professional who does understand statistics and costs, I have to say that the patient clearly should be given the information that can be gleaned from the PSA. The entire concept of not performing the test because it could lead to unnecessary, even harmful treatment, is not what we pay you for.
I want the information and the medical bureaucracy has no right at all to withhold it. The same bureaucracy has been wrong time and again about these topics. I'll make my own decisions, thanks. Just give me the information I need.
Looks like somebody hasn't watched Tropic Thunder.
Ben Stiller:
...is not doubt exactly what he said when he got the test results.
@ Denice Walter: I am seven years out, and I am fine. By the way, that prostate cancer saved my life. It lead to the discovery of an incidental renal cell carcinoma.
@ Sullenbode: I know of no evidence that prostate cancer can be upstaged by a core biopsy, and certainly urologists are doing so many core biopsies that I think such a phenomenon would have been noticed by now. Under certain circumstances, that may be true for other tumor types, particularly sarcomas, but you do what needs to be done in any given circumstance. If you need a diagnosis, and that's the only reasonably safe way to obtain one, you do it and deal with the consequences, if any, later.
OK ... well some of you might be interested to read what read what a Stanford Prof of medical ethics said about PSA screening in 1996 soon after it was widely introduced in the USA! 1996!
“The implication of screening males to detect slow, benign, non-progressive prostatic carcinoma is clear. A test which was epidemiologically perfect (100% specificity, 100% sensitivity) would not, on these grounds alone, be acceptable for screening apparently normal males. The test would also be required to separate males with progressive disease (candidates for treatment) from those with indolent disease (not candidates for treatment).”
He goes on to say: ” In prostatic cancer, only about l/400 patients will show progressive disease. The use of PSA screening could only increase the percent of patients being treated needlessly. ” Should doctors be required to provide that basic statistical fact to patients before they are screened? Or how about afterwards to their potential “active surveillance” patients? Do they even know it themselves? Do they want to know? I doubt it. Their patients then might logically decide to go home and never come back and just skip all those repeat biopsies and blood tests and doctor visits. And even more men might decide to just skip PSA screening in the first place!
And as for unnecessarily telling someone they have “CANCER” and the for-profit medical industrial complex unnecessarily creating millions of new pseudo cancer patients for the rest of their lives via the newly invented term “active surveillance” he had this to say: “Asymptomatic men are urged to undergo a screening test for the early detection of a disease that may well be treated with ‘watchful waiting. ‘ Watchful waiting will result in a large population of men (up to 15,000,000 in the U S alone) (8) held captive by urologists.” … and I imagine the urologists and the oncologists along with the entire for-profit medical industrial complex just loved that idea -- they picked up the PSA screening ball and ran with it as fast as they could ... and dissenting voices like Dr. Robin had to go all the way to India to get his prescient viewpoints published ... and meanwhile millions of lives were needlessly ruined.
The great American pseudo-epidemic of cancer of the prostate
http://ijme.in/index.php/ijme/article/view/1765/3803
Posting the same thing repeatedly is not going to endear you to anyone around here.
Thanks. Wasn't trying to endear myself with anyone. I guess I've noticed that most of you here are entrenched in the "system." Orac seems to have positioned himself as the champion of overdiagnosis and overtreatment more than a little late and AFTER the fact and after the direction of the wind began to change with the USPTS recommendations. Where was he 10 and 20 years ago while all the real damage was being done. Then I see we have here some of his endeared followers with m.d.s after their names still attempting to perpetuate this disgusting (and what should be embarrassing to every m.d. ever involved) bogus prostate cancer epidemic. (I could repeat much of the same about his particular specialty and the mammogram debate that never happened either.
I'll move on and you can be sure that you won't be hearing from me again.
Thx, #33. So different techniques for different tumors; was thinking it would be like this
http://www.cancer.org/cancer/testicularcancer/detailedguide/testicular-…
Ed - promises, promises.
Meantime, there appears to be dead silence about Ben Stiller's endorsement of PSA testing emanating from the bastion of health wackdoodlery, Natural News* (remember, their intrepid reporter(s) have labeled the test a "complete medical hoax"). Can't imaging their continuing to be silent when a celebrity has something good to say about organized medicine.
I apparently missed this gem the first time, but NN got caught selling a "health" product that exposes the public to Evil Formaldehyde.
https://badscidebunked.wordpress.com/2016/07/15/unnatural-news-the-heal…
*I realize this item follows the format of Monty Python's "News For Parrots", i.e. "No parrots died today on the M15 highway".
@Narad #18
It seems to be. Doctors take all kinds of interest in one's colon region after age 50.
Colonoscopy, prostate check.
Which reminds me, I really do need to reschedule mine. They're (as am I) quite interested in viewing my esophagus. I'm willing to place a bet on Barretts esophagus, due to the extreme longevity of GERD and increased frequency/ease of vomiting.
@ Wzrd1:
I would have someone er... look into that if I were you.
I know a great deal about BE because my late father had this condition
( relax, he succumbed to an unrelated condition- VT- at a rather extravagant age)
You can do things ( SBM-wise) to reduce the chance of it progressing to a more serious condition. He did very well despite being over 85 when he learned he had it.
Thanks, Denice. I intend to.
Coughing a few times, such as due to seasonal allergies, results in projectile vomiting. Yeah, I *really* need to get that taken care of. :/
It's on my list...
I began yearly PSA testing in the early 90's because my dad had prostate cancer. All tests were in the low 2s until 2013 when it jumped to 8.8.
My urologist stated that I had probably had prostate cancer for 14 to 15 years and it had only became aggressive recently (it was dx as high stage 2 or low stage 3 depending on the oncologist). I had radiation and chemo in 2014 and two years of quarterly PSA's have been below detection level since. I will now do semi-annual testing for several years.
The good part about having prostate cancer is that it indirectly saved my life two months ago today. Because I had to loose a bunch of weight (200 lbs so far) and that I have been rebuilding my conditioning; I survived my heart attack (less than 7% survival rate). It also helped that I had great medical care along the way.
For me personally, yearly PSA screening didn't save my life until the very end but there were other signs that I had a problem.
I've been told that repeatedly posting things that have been posted already won't endear you with anyone here.
But here we have a poor doctor lamenting the fact that the "public" are demanding their PSA tests!
Be afraid ... be very afraid. "If you are a man you have a 1 in 6 chance of being diagnosed with prostate cancer in your lifetime!. The medical industrial complex cancer fear mongering campaigns all say. Step right up and get your free PSA screening test before its too late. "We care about you." "What about free treatment?" "No ... we don't care that much." "Hopefully you have insurance to cover all the medical expenses you'll likely have after we unnecessarily tell you that you have cancer."
The key word here being "DIAGNOSED." But here's the follow up information that they never ever tell you:
"There are about 380 men with cancer of the prostate for every patient who dies of the disease."
How many "doctors"? People with with "do no harm" m.d.'s after their names? Who should know better? Do you think might have flat out refused to be a part of this scam? How many honest doctors have walked away from any association with it? How many have flat out refused to perform needless "cut it out" surgeries of minor Gleason 6 "cancers" on frightened patients who through no fault of their own were drawn into this fiasco. My experience says its its likely to be a big fat ZERO. Where were the AMA and the AUA on the the unproven benefits of PSA screening right from the start? Promoting it ... thats where they were. (BTW its the same place the AMA is on direct to consumer advertising -- a national embarrassment -- with the same results -- poor hapless m.d.'s being "forced" to prescribe drugs their patients demand as "being right for them."
The 'system" of which they are an integral part of -- sends them these poor uninformed patients -- and they willingly "accommodate" them. Let's see ... should I take the time to do the right thing or should we just get this guy to the OR because that's what "he" wants? (As another poor m.d. commenting on the above referenced blog posts says while shamelessly referring to the insurance reimbursements of his dilemma: "So get the next patient in so we can keep the lights on.")
I hope there is a special place in hell along side the likes of Dr. Mengele for each and every one of them.
Ed @44:
One, step away from the Nazi analogies, please.
Two, you seem to be under the impression that no one dies of prostate cancer. While yes, it is true that most men with prostate cancer will die of something else, there are still plenty of people who *do* die of prostate cancer. So why shouldn't it be treated?
Three, this post was about the risks of overscreening and overdiagnosis, so why are you telling at everyone that too many people are being screened and treated? I'm pretty sure that was the point. What do you want us (or Orac) to say?
So much for Ed's sticking the firmly worded flounce.
Justa Tech @45
One -- the analogy is perfectly appropriate.
Two - I don't know where you got the idea that I thought that no one dies of prostate cancer. But I do know here you got the idea that "plenty" of men die of pc and we ought to be doing something about it! (see #3)
Three -- People do die everyday for all sorts of reasons. Car accidents deaths in the USA every year +32,000, with 2,000,000 injured. Deaths from influenza: 36,000 annually. Estimated deaths from prostate cancer: about 30,000 give or take a few thousand.
The medical industrial complex scare tactics and free PSA screening tout sheets invariably state figures like 30,000 men will be killed by prostate cancer in any given year. Killed I tell you! (Not die of ... its never "die of"). As if each and every one of them could be heroically saved by early detection and treatment ... only if.
But here are some interesting stats from direct from the NCI website: "Between 2003-2007, the median age at death for cancer of the prostate was 80 years of age. Approximately 0.0% died under age 20 0.0% between 20 and 34 0.1% between 35 and 44 1.4% between 45 and 54 7.5% between 55 and 64 19.9% between 65 and 74 40.3% between 75 and 84 and 30.8% 85+ years of age."
So right off the bat we see that most men who die of PC are elderly -- who by any past or current guidelines should never be ethically tested or treated and who unfortunately have to die of something. (But lets also ask the good doctors why a recent study found that 25% of men over 85 were still getting PSA screening?)
According to these stats if you are between 55 and 64 like most people who are caught up in this fiasco -- 7.5% of 30,000 is about 2250 men. 2250 out of a population of about 15,000,000. Just 2250! In reality, prostate cancer is just not a risk worth a second thought. Dying from pc is not even on a par close to that of pedestrians killed crossing the street every year! Don't expect the medical industrial complex to add that complete disclosure to your PSA informed consent form. Neither will it say that there is no possible way to identify these 2250 men in advance -- or that most are simply unlucky and have aggressive PC that likely would never be helped regardless of any amount testing or early detection or treatment.
But cancer scares people. Death from PC can be horrible. The for-profit medical industrial complex has shamelessly pandered to those fears and continues to blow the risks way out of proportion to other more serious risks we face -- harming many men and ruining many lives in the process. And paradoxically it is those very men ...the "survivors"... the 47 out of 48 men who were treated for nothing, many we all know, who also serve to wrongly elevate the perception of PC risk in our minds. The medical industrial complex has created a million man army of "PSA saved my life" dupes who are unaware of the statistical basis of modern medicine and who, along with their doctors tacit consent are only serving to perpetuate this fiasco with their "misery loves company" pronouncements to "get yourself tested." And they all go on to kiss the hands and sing the praises of the doctors who "saved" them. And the doctors eat it up -- all the way to the bank -- and besides, its a good feeling to be appreciated with someone's undying gratitude, however undeserving.
What the fυck are you babbling about?
Ed @47
What on earth are you talking about? I've read your post 3 times and all I can get is that you are very, very upset that anyone is ever tested for PSA.
So, PSA is not the only way to screen for prostate cancer.
More to the point, there is general agreement here that over screening, overdiagnosis and overtreatment are problems! So why are you shouting about it?
And how does pedestrian deaths have anything to do with cancer treatment? It's not like not running a PSA test will somehow prevent someone from walking into the street and getting hit by a bus.
Finally, for you to equate every oncologist and urologist to a evil mass murder is cruel, stupid, nasty and pointless. Would you say that to your doctor's face?
You need to seriously refocus and explain succinctly what you want to change.
Poor Eddie is upset that no one understands him, and we really don't care about his feelings.
A simple G—le search reduces the Bayesian prior rather drastically, but I suppose this is pointless, given that Ed hasn't produced any "tout sheets" in the first place.
Dangerous Bacon @#38
You see ... the way "science" is supposed to work is -- first you do the research and then you do the vetting and then you PROVE the efficacy and value of the screening test and then you introduce it into the population. This very basic scientific method was not followed for either PSA or mammography. And when you initially do stupid things like that and responsible voices looking at the mess its created finally begin to be heard and attempts are made to reverse the damage -- you naturally open yourself to understandable, if misinformed criticism, not only from the likes of Natural News but the Obamacare health rationing conspiracy wing nuts.
Narad @#48
See the comment of the m.d. here:
endearing reposting:
http://scienceblogs.com/insolence/2016/10/10/evidence-based-medicine-gu…
“So get the next patient in so we can keep the lights on.”
Justa Tech @#49
I'll keep it simple stupid.
Prostate cancer is really a non-issue not worth a second thought.
It was made an issue by the marketing departments of the medical industrial complex.
PSA screening continues to do enormous harm with the active participation of doctors.
Eddie: "Prostate cancer is really a non-issue not worth a second thought."
Then why are you here?
“So get the next patient in so we can keep the lights on.”
The only incidence of that quote is from you, which was not referenced to anything. Why should we care about your issues with reading comprehension?
Seriously, this article was about the over testing and over evaluation leading to over treatment. Which exactly what you are complaining about. Did you not even understand that title says "No, the PSA test probably didn’t save Ben Stiller’s life."
Okay, find a dictionary and look up these two words: "No" and "didn’t" (a contraction of "did not"). Then when you are done with that, go somewhere else to clutch your pearls.
Justa Tech @ #49
"Finally, for you to equate every oncologist and urologist to a evil mass murder is cruel, stupid, nasty and pointless."
OK ... maybe the real evil is in that mindless all consuming profit machine called the medical-industrial complex. People can and do rationalize all kinds of things to be able to sleep at night … as I’m sure the guards at Treblinka somehow did — and as I’m am sure many urologists did and still do. They’ve somehow convinced themselves that they are doing the right thing. Before PSA testing urologists didn’t have all that much to do — but since the introduction of PSA, incomes of urology as a specialty have skyrocketed. Somebody got paid for those +1 & 1/2 million unnecessary surgeries these last few years. If a study is ambiguous, as most are, they will interpret it to their benefit. Convinced they are saving lives, the fact that they are making lots of money doing it is just a little side benefit — they see the Wall Street wiz kids making billions shuffling money around — its taken them 12 years of hard work to get where they are — if anybody deserves the big money, its someone heroically saving lives — like they are (even if its only 1 life in 50) ... (and the fact that those other 49 men are patients for life is just another nice side benefit). In my experience talking to many urologists — they are often perplexed when I ask them about one major new PC study or another. Many if not most don’t have the time or interest to keep up with the state of the art and do their own research. They leave all that to their special interest group and cover organization, the AUA (American Urological Association) — Just two weeks after two huge studies in March of 2009 were published showing no benefit to PSA screening, the AUA went charging ahead and changed its guidelines, they completely disregarded all of the science and LOWERED their recommended age for screening from 50 to 40! It was unbelievable! But probably smart … they were well aware that sometimes the best defense is a good offense. They saw the train coming and they wanted to slow it down … or more likely it could just be that over the past 20 years they had completely depleted the 50 and 60 year old patient pool and there were still lots of swimming pool and McMansion payments their members had to make. (They embarrassingly were eventually dragged along kicking and screaming into going along with the USPTS recommendations) Still -- while a lot of harm of PSA screening was being done -- the AUA issued “guidelines” played a big part -- many urologists blindly followed them. It served two purposes — first,they didn't have to do any independent thinking — and second, it provided excellent cover in case they got sued for malpractice.
But eerily “I was just following the guidelines of my profession” does sound a lot like “I was just following the orders of my superiors.”
That excuse didn't work at Nuremberg ... and it won't work on judgement day.
Chris @#55
Oops! I went back and read the title as you advised ... and then the whole article.
Stupid me! Wrong blog! Leaving with my pearls now.
Eddie: "Stupid me! Wrong blog! Leaving with my pearls now."
Good. Buh bye!
Wow, just wow.
Comes here, doesn't read the blog, doesn't even read the title, comments and goes Godwin. Then proceeds to complain about best business practices that keep medical practices open.
Then, goes the rest of the way off of the wire with conspiracy theories and things I have no idea what he was going on about.
Oh well, at least he corrected the initial error of not even reading the title.
Have we been joined by Emily Litella?
Good grief. What a maroon Ed was/is. And, to top things off, he went all Godwin on us. If he honestly *didn't* read the title AND the post before commenting, he's just ignorant.
By the way, Eddie...our host, Orac, gets no money out of prostate screening/surgery. He happens to be a breast cancer surgeon. So all your snipes about him doing unnecessary surgeries on men were just as silly as the rest of your comments.
Also - before you say it - he has posted MANY times, here and his other blog, about overutilization of mammograms to diagnose breast cancer. He's not out trolling the streets and dragging women off to have mammograms, then tossing them on an OR table.
@ Ed Dwulet
Here is the place where you should have put your comments:
http://www.nejm.org/doi/full/10.1056/NEJMp1510443#t=article
Unfortunately, the comments are closed now.
Don't believe everything published in NEJM.
Just Tech @#49
"Finally, for you to equate every oncologist and urologist to a evil mass murder is cruel, stupid, nasty and pointless. Would you say that to your doctor’s face? "
Oh .. I'd go a lot further than that -- if I could find the SOB that gave my dad a PSA test back in 1996 at age 85 as he was happily going about enjoying the last years of his life -- then told him he had incurable cancer and began treating him with Lupron injections -- I'd introduce the back of his head to a baseball bat!
Google: Lupron Medicare fraud
So, I finally got round to reading a bit more on this
According to http://urology.jhu.edu/highlights/2.php (JAMA, 1999), about 35% of men with prostate removal see a rise in PSA after 10 years
http://www.aacr.org/Newsroom/Pages/News-Release-Detail.aspx?ItemID=613#…
Is more recent and seems to make a similar point, that a substantial percentage of men see rising PSA and possible metastic prostate cancer 5-10 years after a prostatectomy
Gleason score and PSA level are associated with recurrence, but it isn't a slam dunk
I think I can stand by my initial comment, that not only does he not know that the cancer would have been fatal if not treated now, he can't know if it will come back.
Maybe "there's a good chance this helped me" would have been better?
Holy..! I think I'm glad it took me so long to see Ed's comment.
Hey Ed - You do not know anything about the rest of the people in the world with prostate cancer. I'm sorry someone screened your dad. Most docs I know wouldn't screen someone that old for anything.
But that has *nothing* to do with all of the much younger men who have been diagnosed, treated and lived. Some of them are diagnosed by feel, you know that? They or someone noticed a lump.
My friend's dad has had 20 more years with his family because he was diagnosed and treated for prostate cancer. My godfather is still with me because he got treated. I know literally dozens of me who are alive now because they actually got treated for prostate cancer. Metastatic prostate cancer.
So you take your "non-issue" and bury it in the backyard.
""I know literally dozens of me who are alive now because they actually got treated for prostate cancer.
That sux. Clones do exibit a high degree of genetic aberrations from the process -- That, and no belly button.
Justa Tech @#66
Future Headline C. 2028 "Ben Stiller says his unnecessary prostate cancer surgery gave him lung cancer"
Let's ask Orac M.D. AMA why there isn't a registry that tracks stuff like this so that men can made "aware" of how badly they are being screwed by the "system" that only pretends "do no harm."
Prostate Cancer Awareness Month my Ass!
You want to trade anecdotes Justa Tech? I know a guy who just had PSA begin to show up in his blood 15 years post his unnecessary prostate surgery at age 58!
https://www.utoledo.edu/med/grad/pa/pdf/Brendan_Boyer_-_JAAPA.pdf
"An elusive tumor in a man who has evidence of prostate cancer metastasis"
G. Shelly @65
See link in #69 Great comment except for your last line. He should have said nothing and kept his mouth shut about his unnecessary surgery and his heroic publicity seeking doctors (who themselves should have set him straight before he published anything). I guessing maybe he was caught drunk driving and his PSA (Public Service Announcement) is part of a court ordered community service sentence. I'm also guessing that his unethical doctors now have a long waiting list of pc surgical patients who want to brag that they had the same m.d. as Stiller.
If I ever finish my PhD thesis on writing styles of the woo-prone and medicine-bashers, there will be a section on inability to bring a sentence to a close.
"Let’s ask Orac M.D. AMA"
Against Medical Advice? Anti-Mitochondrial Antibody? American Motorcyclist Association?* Academy of Model Aeronautics?
*if I had to guess, it's this one. Orac is notorious for his loud pipes.
@DB, way too much information there. ;)
@Ed, oh, how horrible! A patient, operated upon when a specific test was thought to be highly reliable for a very specific cancer, now has, some decade later, a metastatic tumor in the lung, after said original tumor was never located!
Since you suffer from the nirvana fallacy, if you suffer a severe injury, don't go to the hospital - they might screw up. Treat yourself.
his PSA (Public Service Announcement) is part of a court ordered community service sentence
Nonsense! "Psa" is Pseudomonas syringae pv actinidiae, a bacterial disease of kiwifruit that is ravaging NZ orchards.
@Ed Dwulet 65
I will maintain that in my view, overall PSA screening does save some live. There were a couple of papers a few years ago, one in Europe and one in America that generated a lot of discussion at the time, but they did show a benefit. It was difficult, because there wasn't always a standard practice, and certainly, the US and European versions differed (and for the US one, the differences between the PSA arm and non PSA arm may have been so small that we wouldn't expect to see anything even if PSA tests worked)
I found a re-analysis of some of the data (https://www.ncbi.nlm.nih.gov/pubmed/21189374) that for the European one states "they estimated a number needed to screen (NNS) of 1,410 and a number needed to treat (NNT) of 48 to prevent one prostate cancer death at 9 years."
which found very similar numbers,
According to our model, the NNS and NNT at 9 years were 1,254 and 43, respectively. Subsequently, NNS decreased from 837 at year 10 to 503 at year 12, and NNT decreased from 29 to 18.
So, yeah. Unless there is something about his case we don't know, or the numbers for people his age/ symptoms (or whatever) are well established to be different to the general population, it might have saved his life. But there isn't really any good reason to think he would be the one in 20 to 1 in 50 that benefited from the treatment
G.Shelly @ #74
Their is no cure for pc - period -- end of sentence. No one single person diagnosed with pc is ever "cured" by his treatment. Remove a lot of otherwise healthy prostates and you are going to prevent some deaths.
The concept of NNT, is a fun-with-numbers statistical game better suited to promoting the efficacy of drugs not surgery -- has apparently never ever been explained to the legions of "PSA testing saved my life" proponents BEFORE or AFTER their surgeries -- thats because all these unethical doctor's (including Stiller's) stand to benefit financially from the charade -- and besides their inflated "life saving" surgeon's ego's feed on the undying adulation of their conned patients.
Wrzd1@#72
"...after said original tumor was never located!"
You're an idiot who is apparently incapable of reading simple English.
The original tumor was in his prostate which had been removed 11 years earlier after he had a PSA test (his level was only 3) and had been diagnosed with "organ confined" prostate cancer.
How does someone with a PSA of only 3 who has a radical prostatectomy and is told he is "cured" end up with pc metastasis in his lung 11 years later?
@Ed, you're the same idiot that claims that "it's in the living room" is considered precise coordinates.
"In the prostate" isn't precise, within a centimeter or less is precise and hence, a location.
Otherwise, the *entire* prostate is removed and being able to control urine or any other genitourinary function is utterly impossible.
Meanwhile, if it's undergone metastasis, it isn't precisely located, it's "somewhere" in the body and by definition, not located at all, save in the general idea of my car keys are lost somewhere on this damned continent!
I can have a tag that gives a hint that they're on the same continent, but that's it. Nowhere good enough to actually put one's hands on them.
So, who is the idiot? The one that thinks that a found tumor that has metastasised to Christ knows where and he ain't talking, still is precise knowledge of location?
Or someone who recognized that a metastasised tumor isn't local any longer and hence, its location is unknown, even if blood work shows that it's potentially present?
Let me help you a bit.
Tomorrow morning, either take half a usual serving of your usual breakfast of a double helping of stupid flakes and your double heaping slosh of moron milk.
As a tumor not within the prostate could be *anywhere* and still give a positive PSA test. Be it in the big toe or the brain or anywhere in between.
Now knowing that discloses to one and all your usual breakfast, I've given a gentle education, after others have tried to far more gently educate you.
Now, do try to cut down on either the stupid flakes or the moron milk, you might get all three brain cells to actually fire in a more synchronized fashion.
@Wizd1
You're either can't read or didn't bother to read to report. Wzrd1 says:
"... if it’s undergone metastasis, it isn’t precisely located"
" ...that has metastasised to Christ knows where"
"... As a tumor not within the prostate could be *anywhere* "
The report reads:
"However, focal radiotracer reactivity appeared in the upper lobe of the left lung (Figure 1). Chest CT revealed a spiculated lesion measuring 2.8 cm in diameter. The nodular density resembled a primary lung carcinoma; however, the lesion’s location correlated with the area of reactivity seen on the scintigram (Figure 2). Biopsy confirmed that the tumor was a prostate cancer metastasis."
Actually, at the time, I didn't read it, as the network was blocking traffic to that site. Interestingly, I'm at work now (when I'm usually online here as well) and the site isn't blocked any longer.
"Furthermore, clinical evidence of distant metas-
tases develops within 10 years after radical prostatectomy in
15% of patients."
15% isn't especially rare, but it also means that 85% won't have metastatic disease.
"However, lung metastasis with no known bone
or lymph node involvement is extremely rare and has been
described in only a handful of case reports. Therefore, imag-
ing studies of the lungs are usually not warranted when the findings on pelvic/abdominal CT and bone scan are negative
and the patient has no respiratory symptoms."
Also discussed was autopsy results with patients with metastatic disease showing 46% had metastasis to the lung, pelvic lymphatic system and bones, with it being rare to not be present in the lymphatic system and bone, when present in the lung. Unfortunately, there is no mention of the percentage that are so, but it's acknowledged to be a rarity.
So, this is a very, very rare type of case, atypical in several ways.
Well played.