
When I first started to take an interest in medical marijuana, I was struck by how much it reminded me of herbalism. Although herbalism is scientifically the most plausible of modalities commonly associated with "complementary and alternative medicine" (CAM), the use of herbal medicines still involve a number of problems, the biggest of which is what I like to call either the delivery problem or the bioavailability problem. In brief, herbs, when they work, are adulterated drugs. The active ingredient is often a relatively small, embedded in thousands of other constituents that make up herbs, and it’s very difficult to control lot-to-lot consistency with respect to content or active ingredients given how location, weather, soil conditions, rainfall, and many other factors can affect how the plants from which the medicines are extracted grow and therefore their chemical composition. To demonstrate the concept, I frequently point out that it’s much safer and more predictable to administer digoxin to a patient who needs its activity on the heart than it would be for the patient to chew on some foxglove leaves, given that the therapeutic window (the difference between the doses needed to produce therapeutic effects and the lowest dose that will cause significant toxicity) is narrow.
I have nothing against recreational marijuana use and have come around to the view that it should be legalized, taxed, and regulated, just like alcohol and tobacco. Unfortunately, medical marijuana has been co-opted as a "foot in the door" to try to legalize marijuana. The problem with this approach is that it necessitated massively overblown claims for marijuana's health benefits, up to and including claims that it is a great treatment for autism and that it can cure cancer. It isn't and can't. Nor does it stop exaggerated miraculous claims. Basically, the bottom line in terms of scientific evidence for medical marijuana is that it mostly doesn't do what it's claimed to be able to do.
None of this is to say that it might not have some value in some conditions. One condition for cannabinoids isolated from marijuana have shown some promise is in seizure disorders. That's why I learned with interest of a study published in the New England Journal of Medicine (NEJM). This study is a randomized, placebo-controlled clinical trial of a candidate drug isolated from marijuana on severe drug-resistant seizures in children that made the national news Wednesday night. To be honest, the study's gotten less press coverage than I thought it would, but it is an interesting study nonetheless. Medical marijuana proponents frequently misrepresent the skeptic position as being unalterably opposed to the idea that marijuana might have value as a medication. I can't speak for anyone else, but what I've always objected to are the exaggerated, evidence-free claims so many advocates make, and the veritable cult that has sprung up around it. I actually like evidence, which is why this study caught my attention. (Indeed, I would have written about it yesterday, except that the night before I fell asleep on the couch before I got one paragraph in.)
So let's look at the study by Dr. Orrin Devinsky, a neurologist at New York University Langone Medical Center, and colleagues, Trial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome. The first thing I can't help but note is that this is not really medical marijuana, but rather an oral solution of cannabidiol (CBD), Investigational Medicinal Product GWP42003-P, manufactured by GW Pharmaceuticals under the trade name Epidiolex®. GWP42003-P is formulated from extracts prepared from Cannabis sativa L. plants that contain consistent levels of CBD as the principal phytocannabinoid. Extracts from these plants are processed to yield pure (>95%) CBD that contains less than 0.5% (w/w) THC. This pure CBD is subsequently dissolved in excipients with added sweetener and flavoring. So basically, it's a drug isolated from a plant, as many drugs are isolated from plants (and sometimes chemically modified).
Another thing that's important to note is that this trial was to test whether CBD was useful against drug-resistant seizures due to a specific genetic disorder, Dravet syndrome, also known as severe myoclonic epilepsy in infancy (SMEI). Dravet syndrome is due to a mutation in the voltage-gated sodium channel α1 subunit gene SCN1A, which encodes the pore-forming subunit of the NaV1.1 voltage-gated sodium. channel. There are currently more than 700 known SCN1A mutations, and 90% of them occur in DS patients. Two-thirds of these mutations give rise to truncations in the protein while the remaining third are missense mutations that are predicted to severely impair channel function. In patients with Dravet syndrome, the severity of the epilepsy can vary, but myoclonic seizures are the defining feature of Dravet syndrome, and can be massive, contributing to a mortality rate as high as 20% by age 20. The syndrome is also associated with developmental delay. The most devastating aspect of Dravet syndrome is that the epilepsy associated with it is among the most drug resistant forms, and most anti-epilepsy drugs provide inadequate relief.
This trial was pretty straightforward. Basically, it was a multi-institution phase II study carried out in the US and Europe with the following protocol, summarized by this flow sheet (click to embiggen)
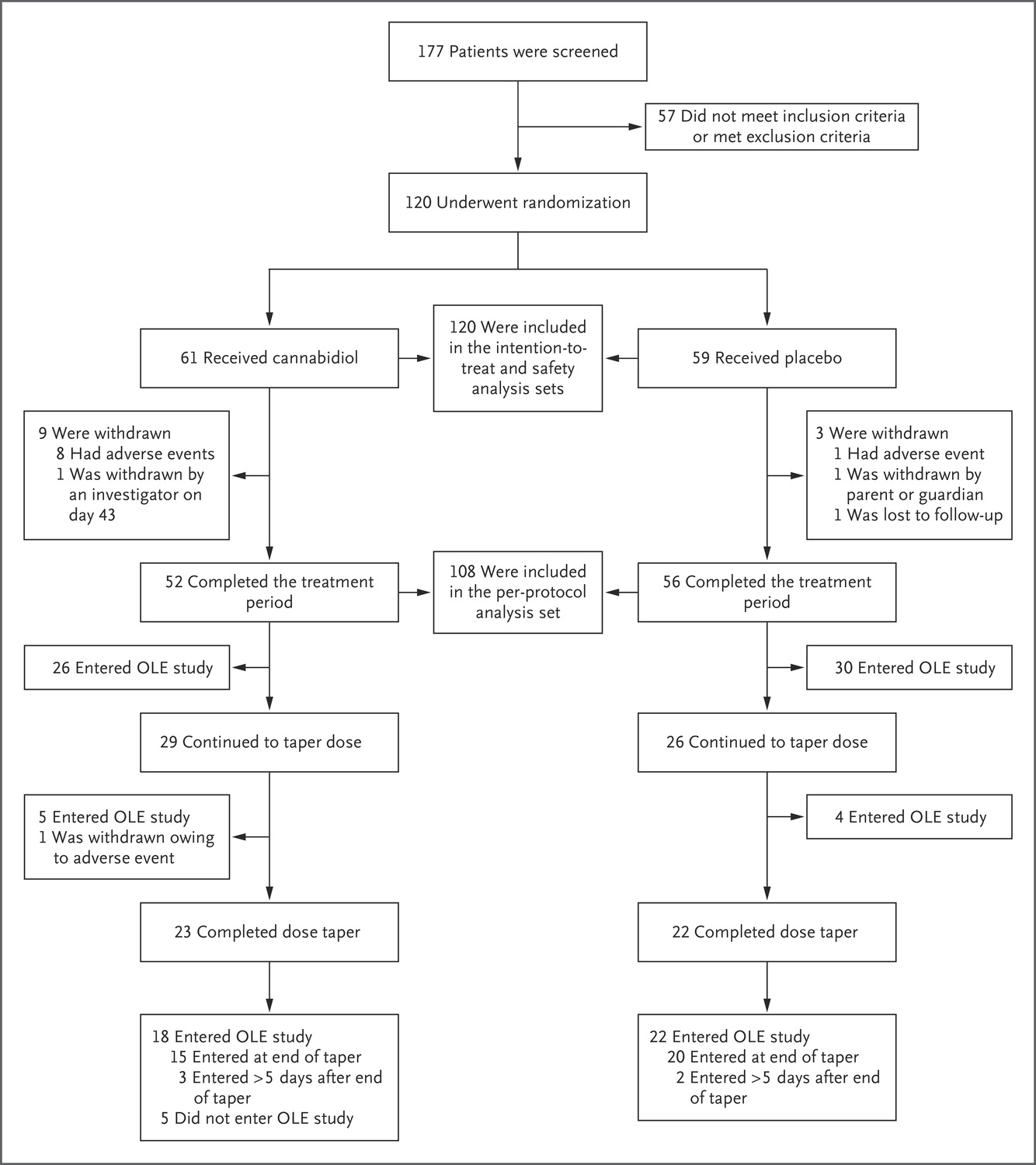
The baseline characteristics of the two groups were well matched, ranging in age from 2 to 18, and patients had previously tried a median of 4 antiepileptic drugs, with a range from 0 to 26(!). Subjects were randomized to receive either placebo or CBD, and the primary end point measured was frequency of convulsive seizures. The CBD solution contained 100 mg/ml, and the placebo solution was identical except for the absence of CBD. Before the intervention began, there was a four week baseline period in which investigators trained caregivers to record daily seizure information. Then CBD or placebo was added to the subjects' regular anti-seizure regimen. This is actually a very important point that most reporting of the trial I've seen misses. This trial does not show that CBD has anti-seizure activity as a single agent, only that, when added to other regimens of anti-seizure medications, CBD can further decrease seizure frequency. We don't know from this trial whether CBD alone would be a useful treatment for Dravet syndrome seizures.
But back to the trial design. The dose was escalated up to 20 mg/kg per day with the use of a 14-day dosing regimen of twice daily administration. At the end of the treatment period, the cannabidiol and placebo solutions were tapered (10% each day) over a period of 10 days. After trial completion, all patients could enter a long-term open-label study. Each day, patients or caregivers recorded the number and type of seizures (tonic, clonic, tonic–clonic, or atonic) for the primary end point. Laboratory assessments were carried out at baseline and after 2, 4, 8, and 14 weeks of the trial regimen, as well as at the end of the taper period for those patients who did not enter the open-label extension study or who withdrew early and tapered the trial agent.
The results were encouraging. In the CBD group, the median frequency of seizures decreased from 12.4 to 5.9 per month, compared with a decrease from 14.9 to 14.1 in the placebo group. The percentage of patients with at least a 50% reduction on convulsive seizure frequency was 43% with CBD and 27% with placebo. The percentage of patients who became seizure-free was 5% in the CBD group, and 0% in the placebo group, but neither of these results achieved statistical significance (p=0.08 for both). I must admit that the way NBC reported Devinsky saying, ""Quite remarkably, 5 percent of the children in the active treatment group with CBD were completely seizure free during the 14 weeks of the trial but neglecting to point out that the result didn't achieve statistical significance. I understand that there were some children who had dramatic remissions, but this observation does have to be put into context.
There were some adverse events due to the CBD, including diarrhea, vomiting, fatigue, fever, somnolence, and abnormal liver-function tests. There were more withdrawals from the trial in the cannabidiol group. Indeed, nine out of the 61 subjects in the CBD group withdrew from the study, compared to only three from the placebo group. Overall, serious adverse events were more common in the cannabidiol group than in the placebo group (16% vs. 5%)
One interesting aspect of this trial is that the mechanism of CBD against seizures in patients with Dravet syndrome is not known. The clinical manifestations of Dravet syndrome are due to a single gene, SCN1A. In an accompanying editorial, Dr. Samuel Berkovic notes:
A major aim in the field of the Dravet syndrome and other genetic encephalopathies is to develop precision therapies — treatments directed at the specific genetic defect. Because the Dravet syndrome has a single-gene basis, it is an attractive target for precision medicine. However, cannabidiol is not a precision treatment for the syndrome, because there is no established link of the cannabinoid receptors with the inhibitory interneuron pathology of the Dravet syndrome, and the response across the cohort of the current study was not uniform.
He also notes:
Devinsky et al. found a significantly greater reduction in seizure frequency among patients who received cannabidiol than among those who received placebo, and the seizure-free rate was 5% with the active drug as compared with 0% with placebo. Thus, anecdote has been confirmed by data, and one might ask whether a controlled trial was really necessary. The answer is absolutely yes. Perhaps counterintuitively, the rate of response to placebo in clinical trials is higher among children than among adults. Moreover, parents who go to enormous efforts to get cannabis for their children report a higher response rate than those who can easily obtain it. Cannabidiol is not without side effects. The dropout rate in the active-treatment group was appreciable, and common side effects included vomiting, loss of appetite, and diarrhea. With additional experience, perhaps these effects can be modified with dose adjustment and other strategies.
I would quibble again here. If you look at Table 3, you'll see that the difference between placebo and control didn't achieve statistical significance for reaching 100%, 75%, and 50% decreases in seizure frequency. Now, I'm not so dogmatic that I won't accept that this difference is probably real, failure to achieve a p-value less than 0.05 notwihstanding, but if you're going to use frequentist statistics and define statistically significant as 0.05, then you should at least be consistent. That quibble aside, I do agree with Dr. Berkovic that absolutely a clinical trial was indicated. I would also add a further quibble that "anecdote has been confirmed by data" is overstating it a bit, given the tiny percentage of patients who were seizure free. However, some patients do apparently have fairly dramatic responses.
Another interesting aspect is that, counterintuitively, seizure frequency did decrease in the placebo group by 13.3%, compared to the CBD group, where seizure frequency decreased by 38.9%. This should be a lesson as to why placebo controls are necessary, even for seemingly objective measures. Of course, given that these were either self-reported or caregiver-reported measures, they are not completely objective; so it is not surprising that there was a slight decrease in seizure frequency, even in the placebo control group.
Finally, I can't help but note that medical marijuana advocates, the ones who will be flogging this study as vindication that marijuana is a miracle drug (even though what this study shows is much more modest) tend also to be very much anti-pharma and pro-alternative medicine. That's why I want to draw attention to this part of the methods section:
The funding source, GW Pharmaceuticals, was responsible for the trial design (with input from investigators and other experts), trial management, site monitoring, trial pharmacovigilance, data analysis, and statistical analysis. GW Pharmaceuticals prepared and provided the active treatment and placebo. Trial procedures were reviewed at multisite investigator meetings. Services were used for clinical laboratory testing; bioanalytical laboratory testing; design of the case-report form; data management; trial-agent distribution, returns, and destruction; the interactive voice-response system; diagnosis of the Dravet syndrome and seizure classification; and translation of documents. The authors vouch for the accuracy and completeness of the reported data and analyses and for the adherence of the trial to the protocol (available with the full text of this article at NEJM.org). The authors affirm that they approved the final draft of the manuscript.
This is, of course, a not uncommon practice for a drug company doing a clinical trial upon which it wants to base an application for FDA approval for its drug, and that's exactly what GW Pharmaceuticals is doing. Nothing wrong with that. It's what a drug company needs to do, and GW Pharmaceuticals is a drug company. It's a good idea to be a little more skeptical about the results of this study than most medical marijuana advocates I've seen gloating over it as total vindication are doing. This is a positive study, but not as strongly positive as it's being spun, and there are issues with CBD and adverse events. As Dr. Berkovic puts it:
This trial represents the beginning of solid evidence for the use of cannabinoids in epilepsy. It requires replication. Future trials may answer further questions about the applicability of cannabinoids to the many other syndromes of childhood epilepsy and to treatment in adults. After an era dominated by anecdote and obfuscated by medicolegal issues and emotionally infused debate, more scientific studies are under way. Much more research is needed to understand the basic science, benefits, and risks of cannabinoids in epilepsy.
Correct. This is a study that demonstrates that one chemical that can be isolated from marijuana has promise as a treatment for the epilepsy assocaited with Dravet syndrome. The mechanism by which it appears to work is not clear, as the relationship between cannabinoid receptor and SCN1A is not clear. It's thus not clear whether this result is generalizable to other forms of seizure disorders, but it's worth investigating. In other words, CBD is just like any other drug. It appears to have reasonable activity against the epilepsy due to Dravet syndrome, but it also has significant side effects, just like a lot of other antiepileptic drugs. It's no miracle, but it could be a step forward, particularly if its study leads to a greater understanding of the role of cannabinoid receptors in seizure disorders.
This a drug combination trial on a constituent of Cannabis sativa L. (not an "ingredient" of the plant because ingredients are items of cake mixes and sundry other inventions rather than nature-made products). What we don't know is whether the results would have been significantly different had the subjects not taken their "regular anti-seizure regimen" in addition to cannabidiol or placebo. We also don't know if that would extend to the adverse events, among which "diarrhea, vomiting, fatigue, pyrexia, somnolence, and abnormal results on liver-function tests" were more frequent among those in the cannabidiol group compared to the placebo group. The fact that more subjects in the cannabidiol group withdrew from the trial than among those who received placebo is at least suggestive of adverse drug interactions. A further question (one I don't expect to be answered any time soon) is what, if any, medications could be dropped from a regular anti-seizure drug regimen without unacceptable harm to a patient with Dravet syndrome receiving cannabidiol?
Well, yes. Most clinical trials these days involve adding experimental therapeutic or placebo to the standard treatment regimen, mainly because in a disease as severe as Dravet syndrome it would be unethical to take patients off of their anti-seizure medications because the placebo group could be subjected to harm. This is particularly true in what are considered vulnerable populations, such as children. A follow up trial in which it is tested whether CBD can allow the dose of other anti-seizure drugs to be reduced would be a logical next step, but it would be tricky to design in an ethical fashion.
It is written,
The dropout rate in the active-treatment group was appreciable, and common side effects included vomiting, loss of appetite, and diarrhea.
MJD says,
Kudos to the brave parents and children in this study.
Q. If the drug proves to be effective, safe, and profitable, will the pharmaceutical company financially compensate those (i.e. test subjects) who sacrificed the most.
In my opinion, medical research subjects should be provided special compensation for their participation similar to our brave soldiers in the armed forces.
@MJD:
While I understand the sentiment behind wanting to richly compensate research participants, it is profoundly unethical to do so. At least when you're talking about reasonable compensation for time, validated parking, and so on. Compensation that's sufficient to become enticing threatens informed consent, by becoming almost coercive to people who need money. That's most of us, but especially people of lower socioeconomic status. And those latter folks are precisely the ones who shouldn't be taken advantage of in medical trials.
Exactly. People will take risks for money that they wouldn't normally take if money isn't involved, and the more money the larger the risks they're willing to take.
In brief, herbs, when they work, are adulterated drugs.
No, they are "impure" drugs, but not "adulterated" because nobody added anything to make them impure. They grew that way from the start.
That distinction may matter in a legal context, but in a medical context, it's to-MAY-to vs. to-MAH-to. The patient is getting a drug in an unknown (to him) dose with unknown (to him) additional compounds that may or may not help with the delivery, and in some cases may interfere with it. If said patient ends up dead, it won't matter to him whether the product was represented to him as an herbal product or as a drug of claimed dosage and purity. The lawyers who take on any subsequent wrongful death case, of course, will care.
Thank you for giving this very, very careful and nuanced explanation. It really helps understands the strengths and limits of the trial.
Thanks for this! I watched the CBC coverage and nowhere was it explained that the CBD was in addition to the regular meds. It was presented as marijuana the saviour drug. And some irritating patient activists leading the way and science catching up narrative.
I'm not sure where the parents got CBD in Canada, my wife can only get Sativex here (a 50:50 CBD:THC med). If it is from the current medical marijuana dispensary world, who knows what they are giving their child.
Now appears to be a good time to remind people how much I hate pedantry and how much it irritates the hell out of me. If the word "adulterated" bothers you so much, I'll just change it to "impure." The specific word used, as Eric points out, doesn't much matter for purposes of the idea, nor does it matter much in a medical context. The point is that there are hundreds, if not thousands, of compounds mixed in with the actual active ingredient of an herbal medicine.
It should be noted that only the kids who were also taking valproate (a seizure medication) showed elevated liver enzymes -- Something Vaproic acid can do all by itself.
What else would it be? Millions of people anecdotally know how it helps them. When a study is finally allowed it showed the users were right.
"counterintuitively, seizure frequency did decrease in the placebo group by 13.3%, compared to the CBD group, where seizure frequency decreased by 38.9%"
I agree this is a reminder of the importance of placebo groups, but I expect the placebo response in this case has more to do with trial participants stepping up their compliance with their usual meds during the trial as opposed to succumbing to bias on subjective symptom scores.
Gilbert @7: Speaking to the issues of lot-to-lot (or crop-to-crop) variability.
Are you a wine person? If so, are you familiar with the concept of terroir? (The idea that you can grow the same grapes in two different places and things like the mineral composition of the soil will affect the flavor of the wine.)
It's a lovely thing, in wine or in tomatoes or cheese. But you need to remember that while that variability is often wonderful, producing glorious vintages, it can also produce crap that's not even worth putting in a bottle.
If I gave you a glass of a clear beverage you'd want to know if it was pure water or pure ethanol or something in between. And if it's something where you can't tell the difference *before* ingesting it, then it's even more important to know how much you're getting.
And what's wrong with testing and labeling? In the recreational sphere it really broadens the market. Where some might say "I feel like a rose tonight" another might say "I'm feeling like a X% THC, Y% CBD tonight".
But medicine is all about precision.
Where did you find this? Is it in the full paper?
I haven't seen the paper. but I assume that's where this comes from:
https://arstechnica.com/science/2017/05/marijuana-component-reduces-sei…
Some of those kids rotate amongst ten anti-seizure/epileptic drugs including phenobarbital -- None of which work. I'd think the next studies should be to treat those patients with only CBD and with a complementary inclusion of THC for suppression of nausea and increased appetite.
I would not be surprized if continuing the drugs hides the true effectiveness of the clean-acting CBD alone.
@ Gilbert,
Yes, valproate can raise liver function tests, and cause hepatic toxicity. That's why a baseline should be taken when you start it, and it should be monitored regularly for the first six months.
If you then add another drug and LFTs rise, it is more likely the second drug is the contributing factor. You have to consider if the problem comes from the second drug, or the fact the two drugs are combined before you decide how to change the treatment plan.
In this study, participants were in a four week baseline period before beginning the cannabinoid or placebo. In order to establish that baseline, and perform the regular checks during the trial itself, bloodwork is done. The LFTs of the patients who left the group (only 3, btw, with one from the placebo group) rose after starting the CBD treatment. The other nine patients completed the study in spite of the elevated liver enzymes.
What this means is there may be reason to believe that there is additional risk of adverse liver issues for patients taking CBD who are also taking valproate. The answer is dose adjustment. You cannot conclude that the problem is the valproate and not the CBD, or that CBD is automatically safe if the patient is not on valproate.
@Johnny: yes, the full paper does in fact note that the only patients who had elevated LFTs were on some form of valproate.
I take it, Eric Lund, that your statement is a generalization of all herbal medicine and not to intimate that could become the case with MMJ.
Otherwise, I challenge anyone to find one death attributed to cannabis** in ten thousand years of recorded history.
** Of course, not the synthetic 'legal high' THC which can be fairly deadly.
Orac, please, PLEASE cover this.
Open Access Journal, apparently 1.4 impact factor, case studies, alleging marijuana causing violence. ("Violence is a well-publicized, prominent risk from the more potent, current marijuana available. We present cases that are highly popularized storylines in which marijuana led to unnecessary violence, health risks, and, in many cases, both.")
The case studies include a handful of people who were shot by cops or others (Michael Brown, Trayvon Martin), the guy who shot up the Co. Planned Parenthood Center, the Boston marathon bombers, and OSAMA BIN LADEN.
One of their first sentences, "Marijuana intoxication results in panic reactions and paranoid feelings whose symptoms lead to violence " has a citation that turns out to be, something the NYPD Commissioner said. (something stupid).
I would tear this to bits, but I don't have the patience, stamina, nor knowledge to do it.
https://www.omicsonline.org/open-access/marijuana-violence-and-law-2155…
Can anyone explain why these studies, and everyone moving and getting in a queue to acquire charlotte's web, go after >95% cbd oil product offerings extracted from recreational marijuana strains vs the non-recreational strain, aka hemp, that naturally has that level of cbd. Currently you can buy 25-30% concentration cbd oil tubes produced from commercial hemp online w/o any medical marijuana referral/license required and for much less that equivalents produced by multiple solvent + other procedures applied to recreational marijuana.
Osama Bin Laden? What a bunch of maroons. You can't get marijuana in Pakistan or Afghanistan.
CJTX, if ORAC did a critical review of every dingbat article published in a pay to publish journal, he wouldn't have time for his day job, or sleep. All his blinking lights would burn out, leaving a dark void.
The lads at Wikipedia beg to differ
https://en.wikipedia.org/wiki/Cannabis_in_Pakistan
"Cannabis is widely used in Pakistan..."
https://en.wikipedia.org/wiki/Cannabis_in_Afghanistan
"Cannabis in Afghanistan has been cultivated for centuries..."
@Panacea - thanks for the info.
Johnny: Huh. I assumed it was forbidden, and also impossible to cultivate at high altitudes.
I would tear this to bits, but I don’t have the patience, stamina, nor knowledge to do it.
Author is a Professional Expert Witness grifter. Paper is basically an advertisement for his services. The litany of high-profile cases of police and vigilantes shooting black kids is so he can invent an encounter with marijuana for each of the victims, and argue that that encounter turned them violent and scary (and black) so that the police / vigilantes were compelled to shoot in self-defense. So the author is shamelessly self-whoring announcing his willingness to testify in the defense of uniformed lynchers in the future.
Any decent journal would only have published the piece with a label of "Advertisement", forcing him to resort instead to the negotiable standards of an OMICS dumpster.
CJTX:
We present cases that are highly popularized storylines
That is not a sentence intended to be read by scientists. The authors are writing for an audience of defense lawyers who need a simple narrative to absolve their clients (by blaming their client's victims).
I am going to hazard a guess that nine times out of ten, when someone is trying to pretend that marijuana causes violence, that person is an apologist for police violence or increased powers. The authors are advertising their services to cash in on future police violence.
You need to learn not to assume so much, grasshopper.
Given that there was a higher dropout rate for adverse events in the CBD group, how can researchers control for the possibility that the dropouts were somehow more likely to be unresponsive to the CBD treatment, thus making the average effect higher due to removal of low/no responders from the CBD group?
One scenario I can imagine is that those receiving a benefit from the CBD could be more likely to stay in the trial when experienceing side effects that those not receiving any benefit (I.e. Getting a treatment effect is "worth it" to stick it out, but if you're not seeing any benefit, you wouldn't consider it "worth it" to stay in the trial).
With the sample size, the difference between losing 9 patients in the CBD group versus 3 in the placebo group could make a difference.
Or is this something that researchers can control or account for?
"Unfortunately, medical marijuana has been co-opted as a “foot in the door” to try to legalize marijuana."
This is a logical consequence of (wrongly) classifying Cannabis as drug with no medical uses or benefits and using this in a legal circle jerk to justify its prohibition.
"The problem with this approach is that it necessitated massively overblown claims for marijuana’s health benefits..."
In a hypothetical sane world, one demonstrated medical use would be enough to trash that wrong classification. This didn't happen, so now you have Anslinger's Devil Weed with flipped sign.
Just a note: Sorry to all the regulars who got stuck in automoderation because they had been impersonated by a certain sock puppeteer and I have to make sure it's you before letting you post. I had visitors yesterday, and I was away from the computer for nearly 16 hours, which means a bunch of you didn't get your comments posted until just now. I'll try to keep a better eye out.
I will, however, mention that I'll be on vacation in early June. I haven't decided yet how much (if at all) I'll be blogging or whether I'll be posting "reruns" or a mix, but the time is fast approaching for me to make up my mind...
It touches on JustaTech's "lot-to-lot (or crop-to-crop) variability".
The Stanley brothers' Charlottes Web is pretty standardized: It is tested, it is grown in a controlled environment, and propagation is through cloning.
Please have some good vacation time Dr Orac :)
Alain
madder (#4) says,
... but especially people of lower socioeconomic status. And those latter folks are precisely the ones who shouldn’t be taken advantage of in medical trials.
MJD says,
Q. Can monetary awards for trial participation increase the placebo effect (e.g., placebo currency) in people having a lower socioeconomic status.
If the answer is YES, placebo currency may be a confounding variable and should be eliminated to control the validity of the experiment.
Alternatively, if placebo currency (i.e., integrative medicine) has efficacy it may be a useful supplemental treatment for needy individuals having lower socioeconomic status.
Are you suggesting, like Chairman Mao, that sometning like acupuncture is good enough for the peasants? Because I thought you were just an idiot and a loon, but this would move you into the 'evil SOB' category.
PGP @24
Go figure.
Could you try to learn from this one, please ?
Sorry to all the regulars who got stuck in automoderation
I WANT MY MONEY BACK.
@ Gilbert #16: What you posted in reply to my comment (which got moved to #17 because of the posts that went into automoderation) is called "shifting the goalposts."
That some of these kids rotate among a variety of anti-seizure medications has ZERO bearing on my response to you, or on the 3 kids who dropped out of the study due to increased LFTs. It only matters what the kids were on AT THE TIME.
And you can't wave your magic wand and say phenobarbital doesn't work when in fact it does, or that even if it actually didn't (which is a falsehood) that somehow magically means CBD is safe.
Citing an Ars Technical review of this paper which essentially says similar things to what Orac says without the insolence doesn't support your point in the least.
This study hasn't proven CBD can control seizures by itself. It only showed a reduction in the number of seizures the child had. Considering that seizures can be life threatening, simply jumping to a CBD only study as you suggest is premature. It is unethical to withhold treatment that works just to test a pet theory.
The authors believed the increased LFTs were due to a drug to drug interaction with valproate. They also believed since most of the kids taking valproate remained in the study, and also based further blood work, that this interaction was temporary. That needs more research; if so it simply means that most kids would be able to remain on valproate while taking CBD.
Odds are if these study findings are confirmed, CBD might become an adjuvant therapy for kids with Dravet syndrome who are not as well controlled on other drugs as they could be. We're years away from proving it works on its own and can be a primary therapy.
Also, we have no long term safety data on CBD alone, as the authors acknowledge (and you ignore). If something pops up with chronic use over time, that will limit its usefulness.
I was not replying to your comment as I commented first. That's what #16 comes before #17 means. Though I saw your comment well before my moderation kicked out -- ORAC's tiered moderation methods to 'slow you down' I take it.
Moving goalposts. Hmm. I seem to recall that Charlotte Figi went from 300 seizures a week to one and that they had stopped all the other meds -- It was 2013 when I heard the story so I may be wrong.
Johnny (#34) writes,
Because I thought you were just an idiot and a loon, but this would move you into the ‘evil SOB’ category.
MJD says,
My comment about "placebo currency" was intended to bring transparency to the potential benefit of a post therapeutic-intervention for test subjects. :-)
Your respectful insolence is like holding a skunk by the tail, it's always unpleasant.
@ Alain (#32),
What's a nice person like you doing in a place like this?
Understand, you'll always be a pseudo-minion in Orac's dominion.
@ Orac,
If your VACATION, in the month of June, takes you to a foreign country will you be fully vaccinated?
In the absence of a response, we will assume that you are a closet antivaxxer.
@Gilbert: I can't help it if you don't pay attention. My #17 was posted before your #16. Perhaps you were replying to Johnny but you didn't make that clear. You still shifted the goal posts.
Charlotte Figi's ONE case isn't evidence of anything. What it did was spark interest in real research on the subject, which is now being done. Her case is still anecdote, not data, though if true I'm certainly delighted to hear she is doing better.
MJD: we don't understand completely why the placebo effect happens. Lying to patients is unethical, and right now we have to lie to patients to deliberately trigger the placebo effect. The effectiveness of doing that is dubious at best, and allows people to continue suffering at worst which is not cool.
But then again, you've proven time and again that ethics don't really concern you, so I'm not really surprised you'd advocate this.
Poking the bear is not funny. Better watch out he doesn't bite your head off.
@MJD:
The potential confounding factor presented by financial incentives to trial participation is a good reason to continue avoiding those incentives. And while I won't respond with quite the vitriol as Johnny did, I do wonder if you've thought through the ethics of your proposal to focus placebo treatments on the less fortunate, coupled with financial incentives for them to participate in clinical trials. You can't possibly be serious, can you?
I mean, just wow, dude.
Panacea (#40) writes,
But then again, you’ve proven time and again that ethics don’t really concern you, so I’m not really surprised you’d advocate this.
MJD says,
The other day an unhealthy-looking homeless man asked me for $ to get a smoke.
His teeth appeared like buttered corn as he smiled and gave a hearty thanks for the $.
In my opinion, the placebo currency-effect is real.
And I can't help it if you don't know how moderation works, I was replying to Johnny. Though I did see your comment was published first shortly after I subitted mine; I doubt you were ever in moderation.
Ohh. my bad. comment #15 was
To which I replied
I guess that is a little bit ambiguous to you. Again, #16 was submitted before #17 was posted. Silly.
Have a great and well deserved holiday, Orac.
MJD - If you are indeed proposing 'placebos for the poor', then yes, I stand by my statement that you are an evil sumbitch, and I've a feeling I won't be alone.
I really don't understand your post #33, and #39 didn't really help.
Well, fine. You got me Gilbert. I misunderstood who you were posting you.
Enjoy it. Everything else you said is flat out wrong.
This is why you can't get kif in Morocco, either.
I've heard tell that some of the best and smoothest cannabis comes from arid conditions at moderate elevations. The plants thrive with plenty of water but the dry air reduces degredation of the cannabonoids as they are formed and the elevation increases UV which also enhance cannabonoid production. All and all, the same strain will come out better in Afganistan than in the muggy conditions of the southeastern US or even mexico.
Panacea, you qualify for the *find a death after ten thousand years of recorded history challenge*.
http://www.huffingtonpost.com/2013/09/03/marijuana-deaths_n_3860418.html
And that ^ is from carbon monoxide poisoning.
The "dose adjustment" is use until the desired effect is achieved as there is no toxic dose from the constituants of cannabis.
MJD,
this place, i enjoy.
Orac, that's a job requirement that he be fully vaccinated according to the standard of care. Never mind travelling (which may carry some recommendations).
Al
Gilbert: while no one has died directly from an overdose of cannibis . . . yet . . . they have died from being under the influence, often while driving or some other mishap where they would not have died had they been sober.
I say yet because with the increasing levels of THC in the cannabis being produced today, once of these days we will find out what the lethal dose is . . . probably the hard way. Too much of anything is bad for you, even water.
And even the milder forms of pot our grandparents used in the 60's still had side effects. We know that chronic marijuana use in teenagers has adverse impacts on brain development. In sort, cannabis may be "safer" than many other drugs people use, but it is by no means benign.
I support legalization, by the way. The reasons for making it illegal were always bogus to begin with, and even with its known problems, alcohol and tobacco are worse in many ways.
But we're talking about using cannabis as medicine. A different standard applies. What I said about dose adjustment still stands; your blather about toxicity doesn't change the fact that we already know from the study under question that combining CBD and valproate can raise LFTs. That's worth knowing about cannabis, since many people combine it with other drugs. The likelihood that people who take it for medical purposes while taking zero other drugs is pretty low.
And this study still hasn't proven CBD safe or effective for anything, not even Dravet Syndrome. It's proven it may be effective . . . safe is still an open question, and only in a limited circumstance. More research is needed, especially since so many other studies of cannabis have been unconvincing.
Alain (#51) writes,
...that’s a job requirement that he be fully vaccinated according to the standard of care.
MJD says,
In an article from Lexology (2013) titled, Firing employees who don't get flu shots: what risks do hospitals face?, author Mark D. Nelson writes, "Hospitals, of course, have reached different decisions on how to balance the interests of patients and employees. As such, policies vary in the flexibility given to employees regarding non-vaccination and the resulting consequences:
Vaccination mandated with exemptions for medical contraindication, religious beliefs (discipline/other adverse consequences for non-exempted employees).
http://www.lexology.com/library/detail.aspx?g=d47d4235-8619-4bbe-aa16-e…
Q. Why are non-exempted employees singled out for punishment/other adverse consequences.
@ Orac,
Are you a non-exempt employee at the hospital?
My apology for the off topic question(s) about vaccination but it seems particularly-relevant knowing that Orac may be taking a vacation in early June, 2017.
@ Orac,
In the hypothetical:
If you are going to Mexico for some R&R, is it your responsibility, as a cancer surgeon, to protect your patients and determine the flu risk from the World Health Organization (WHO) before departing?
http://www.who.int/influenza/surveillance_monitoring/updates/latest_upd…
Please advise...
@Panacea #52
I suppose those are some good points.
MJD- you really are a bulldozer in a china shop - i assume Orac is intelligent enough to get any shots required for an overseas vacation like every sane person. He might be enjoying a "staycation". He might be going to Lost Wages or some other US tourist attraction. What business is it of yours?
You seem to be suffering from a fantasy that you can weasel out a confession that he hasn't had his shots (and therefore is a secret antivaxxer and hypocrite) . Not going to happen. Give it a rest.
Pretty pathetic.
Jane: not to mention MJD doesn't seem to know what non-exempt means.
Jane O. (#55) writes,
What business is it of yours?
MJD says,
It's none of my business, although, in the spirit of full disclosure it would behoove Orac to come clean about his vaccine history before any of us jump on his bandwagon.
Personally, I want to believe that Orac practices what he preaches.
@ Orac,
What say you?
Note: Verification of vaccinations, including those based on foreign travel, for the past 10-years will be adequate.
One might recall that this was a favorite of ol' Gerg's, as well.
Chemmom :Ok, ok. I'll stop commenting and lurk here quietly Right after this.
Narad: I wouldn't know about the drug scene in Morocco. Never been,and I'd be more interested in the wildlife.(Heck, I can barely tolerate tobacco.)
MJD: Do you understand seasons? Flu is more prevalent and virulent in winter and fall. Orac is travelling in summer. Even during 1918, there were very few outbreaks during summer-well, until late August-early September. So you're chicken littling about a very tiny risk to his patients and Orac himself. Not to mention that hospitals provide free flu vaccinations every year. Why do you assume Orac is too dumb to take care of himself?
This 'I am the only intelligent lifeform on the blog' posture of yours is getting beyond stale. It's even staler than Gilly's hippy-dippy 'I want all the drugs' policy.
OK, Panacea, an earlier study suggests the combination can be a problem. Maybe it does act like grapefruit does with some drugs:
https://www.scientificamerican.com/article/can-cannabis-treat-epileptic…
PgPig (#60) writes,
So you’re chicken littling about a very tiny risk to his patients and Orac himself.
MJD says,
I would never downplay a flu virus and recommend regular flu vaccinations, when available, independent of the season.
I'm surprised to read your comments, PgPig (#60).
I hope Chemmom doesn't put you back on a short leash after that outburst and/or effort. :-)
MjD - Think about it - why would anyone in their right mind waste one second of their time rummaging through their files to verify to a stranger in the "interwebs" that they have had their vaccinations?
I believe in Pap smears, but i wouldn't feel the need to prove to some random jerk that I've had mine regularly.
I assumed [Marijuana] was forbidden, and also impossible to cultivate at high altitudes.
I guess that rules out the usual explanation for the name of Hassan-i Sabbah's group, the Hashshashin.
I'm not our host, but challange accepted. Copied direct from my HMO website. True, honest and complete, you have my word on it, but, of course, how do you know? And just what exactly is this suppose to prove?
Immunization
Date
INFs 3yrs-adult (Influenza)
10/10/2009, 10/7/2007, 10/21/2006, 11/6/2005
INFs 4yrs-adult (influenza)
10/4/2008
INFs pres free 3yrs-adult (FLUARIX Quadrivalent) (Influenza, split virus)
9/9/2016, 9/17/2015
INFs pres free 3yrs-adult (Influenza)
10/17/2013, 9/14/2012, 10/11/2011
INFs pres free 4yrs-adult (FLUVIRIN) (Influenza)
10/21/2014
INFs pres free 9yrs-adult (AFLURIA) (Influenza)
10/19/2010
Tdap (ADACEL) (Tetanus, diphtheria, acellular pertussis)
7/27/2010
ZOS (Zostervirus live, shingles)
11/29/2016
Jane O. (#62) writes,
- why would anyone in their right mind waste one second of their time rummaging through their files to verify to a stranger in the “interwebs” that they have had their vaccinations?
MJD says,
Understood, let's all agree that Orac has and will always be vaccinated.
@ Orac,
If you miss one or many vaccines hereafter, you'll still have my/our full support.
Johnny (~#64) writes,
And just what exactly is this suppose to prove?
MJD says,
Good character from you Johnny and if Orac made such an effort we would all benefit knowing he's doing the right thing.
Gilbert: The possibility of a drug to drug interaction is present with every combination of drugs that exists.
Jane: regarding MJD. Agreed. he tries to come across as funny, and only manages to present himself as smarmy.
If Orac posted his vaccination information like Johnny, no, we would not all benefit. How is that information a benefit to any stranger? I assume he has done everything sensible and necessary (like normal people who are not antivaccine nuts) and i don't need to have this verified.
Christ you are paranoid.
I disagree. I would suggest that if this quote reflects your actual belief, it proves you have a very low bar for persuasive evidence (which I believe everyone here already knows).
While my post above is a true and accurate copy of my shot records for the last few years, there is no way you could know that. If you accept it a face value, you are a foolish person (and no, I will not post my HMO login info so you can check up on me).
To answer my own question, all it proves is that I can look up which shots were given in a particular year and make up a few dates. If our host was to post his 'records', it wouldn't prove a darn thing either.
Your challange was a silly thing, and you should feel bad for posting it.
Jane O. (#69) writes,
Christ you are paranoid.
MJD says,
Having been publicly flogged by Orac as an "Anti-vaccine Zealot" and thereafter regularly placed in auto-moderation, it is my intent to provide personal comments that do away with such anti-vaccine rhetoric (i.e., judgmental insolence).
A respectful and productive conversation on the risk/benefit ratio of vaccines can only be accomplished in the absence of any form of insolence.
@ Orac,
Please consider renaming the much frequented Scienceblogs Respectful Insolence to "Respectful Judgment".
A smidgen of harmony and cooperation MAY ensue thereafter.
I don't know how many of those making comments here have any personal experiences with seizures or epilepsy,but I have lived with recurring/relapsing seizures for decades.In the last few years,they have been mostly atonic,and have gotten worse.I have several underlying genetic and medical issues,involving multiple systems.metabolic,autoimmune,and neurological.
In complex cases like mine,it can be very difficult to say what is the underlying cause of the seizures can be.Standard antiepileptic drugs can often cause more seizures, or make existing seizures worse.As with other conditions,such as MS or cancer,I think there is a lot in favor of a right to try here.Especially if we are talking about CBD oil derived from cannabis,with the THC removed,something I very much do want to try.
We all know there are too many scammers out there who just want to get high,and too many enabling doctors,with questionable credentials,that will gladly create a phony PTSD diagnosis for these scammers,but there can be legitimate reasons to try products derived from cannabis.Whether or not this is actual medical marijuana,is debatable.
Yes, it was first *assumed* that the infected machines were probably XP because, as it is no longer supported, it did not get an update.
Since then, analysis has shown the vast majority of infections were win 7 machines. Though they finally did roll out an update for XP. In fact, I'm suspicious -- NSA lost some tools; They want to implant new ones.
It should be noted that WannaCry was just the current payload of the exploit ETERNALBLUE. It may be that win XP is off the radar because they bluescreened before the implant could activate.
https://arstechnica.com/security/2017/05/windows-7-not-xp-was-the-reaso…
And the beat goes on.....
Oh man, is my face red. I just commented on the wrong website; please ignore.
As for pot, "CBD is a potent liver enzyme inhibitor it can increase the concentration of other drugs in the body. This means that when administered with other compounds, consequent effects on patients may be due to the increased exposure to those other drugs rather than the CBD itself." (#61) -- makes sense then that there were side effects because the patients may have been effectively overdosed on their regular meds.
No worries Tim - I actually liked both of your comments.
e marijuana in Afghanistan and Pakistan
Whilst I have NO idea about it...
I'm sure that they have other more lucrative drugs sources to plant that bring in REAL MONEY
Hi, Tim: In essence, yes. Dosing and frequency of medications is based on the goal of maintaining a steady therapeutic serum level. If a drug to drug interaction causes something to take longer to metabolize, then it can cause a higher (or lower) than desired serum level, with the accompanying additive effects.
This is why people on coumadin shouldn't take St. John's Wort.
In this case, though, the issue is the effect on metabolism. Valproate is metabolized in the liver. So is CBD. In addition to potentially increasing the action and effect of valproate, the combination is stressing the liver somewhat, to the point where three participants in the study had to drop out, while nine others were able to continue.
So it begs the question; is the action of CBD in the liver somehow complimenting the action of the other anti seizure medications in a desirable way (making it useful as an adjuvant therapy), would it be useful on its own as a treatment, or is it simply going to complicate current therapies. The answers to those questions aren't answered by this study. More research is needed.
@Roger: my sister suffers from a very odd form of a focal seizure that causes arm, shoulder, and neck spasms, always the same side and direction. Overstimulation is a trigger; she often gets these when she is tired, when we've been to the movies or is under some other kind of stress. She also has fibro myalgia. She uses pot (medical marijuana is legal in our state, with a vaporizer, as I warned her not to smoke it) when she has a "fibro flare up" to deal with the pain. It works for that quite well, but puts her out like a light so she only does it at night when she's home.
It's had no impact on her focal seizures that we can see . . . and she keeps up with the research into medical marijuana (and is a skeptic herself) because of how the subject impacts her directly. She's well aware of the claims, doesn't think it helps her for that.
MJD @3: Clearly you have never taken a bioethics course, because pretty much lesson 1 is that you can not give anything of real value to study participants because it interferes with/negates their consent.
(Example: "I'm not sure about this study, but I really need to make rent this week." That's coercion.)
Too many parents who gave their children CBD oil which is in hemp and pot; stopped all their seizures and many stopped using their normal medications.
But if CBD is not POT then why did the DEA ban hemp and CBD oil?
If you're taking this site serious, consider a new source of information. You're being lied to; special interest have many interest in only curing symptoms and not disease.
It's the basis of corporate greed and crony capitalist. Why are you going to run yourself out of business? Money always wins; greed always wins.
The truth will remain elusive for the majority who rely on centralized sources of information. 90% of media is controlled by 6 corporations.
"Earth"
Are you sure? Have another look around you.