
 There is an article about cancer in this month's issue of Scientific American written by pioneering the virologist, Peter Duesberg. For those of you to whom his name sounds vaguely familiar, Duesberg became famous by claiming that HIV doesn't cause AIDS. Fortunately, this article does not go into his radical ideas about HIV. Instead, this piece explores his more plausible hypothesis regarding the cause of cancer, which proposes that the source for many cancers is aneuploidy: a condition where the cell's chromosomes are scrambled -- duplicated, broken, structurally rearranged or missing entirely. In contrast to Duesberg's unconventional ideas about the HIV-AIDS connection, his argument is compelling for the link between this observed chromosomal chaos and cancer. I thought you would enjoy reading my summary of this article since the original is behind a subscription wall.
There is an article about cancer in this month's issue of Scientific American written by pioneering the virologist, Peter Duesberg. For those of you to whom his name sounds vaguely familiar, Duesberg became famous by claiming that HIV doesn't cause AIDS. Fortunately, this article does not go into his radical ideas about HIV. Instead, this piece explores his more plausible hypothesis regarding the cause of cancer, which proposes that the source for many cancers is aneuploidy: a condition where the cell's chromosomes are scrambled -- duplicated, broken, structurally rearranged or missing entirely. In contrast to Duesberg's unconventional ideas about the HIV-AIDS connection, his argument is compelling for the link between this observed chromosomal chaos and cancer. I thought you would enjoy reading my summary of this article since the original is behind a subscription wall.
Duesberg's group arrived at their hypothesis by rethinking the basic biological features about what makes a human cell "normal," or even "human." Basically, individual genes can be quite variable within a species but chromosomal structure is not. For example, the genes for eye color can encode a variety of colors from one individual to the next, but the actual genes for eye color are always found on precisely the same location on exactly the same chromosome in every individual of the species.

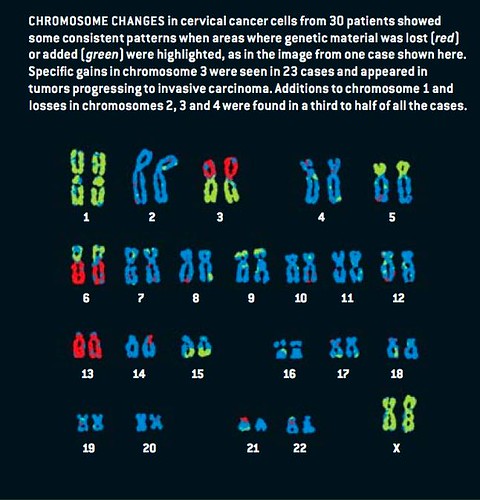
A normal human somatic cell is diploid; it carries two complete sets of each chromosome (pictured, above). However, solid tumor cells are not diploid. According to the author, cancer cells are always aneuploid -- hosting one or more severely damaged, missing or extra chromosomes. As a result of aneuploidy, the total DNA content of a cancer cell can either be more than twice or less than half of what is found in a normal cell. This imbalance makes the cells cancerous because they cause the cell to produce wildly skewed amounts of those proteins that are encoded by the thousands of genes that were either gained or lost. This disrupts normal functioning of these cells, leading to cancer.

Because of their structural complexity, the most vulnerable proteins in the cell are those that comprise the mitotic spindle fiber apparatus that is responsible for segregating chromosomes during cell division. The failure of the mitotic spindle fibers can cause aneuploidy, thereby contributing to additional derangements of chromosome number (see above and below).

Abnormalities in the spindle proteins reveal how cancerous cells within the same tumor can exhibit different combinations and alterations in their chromosomal make up, or karyotype. This variance in karyotype effectively makes each cell a new species. Further, this inherent instability also allows individual cancer cells to evolve new traits and behaviors, unlike normal cells in an organism, which are destined to develop predetermined characteristics depending upon the organ or tissue type they belong to. Thus, an aneuploid cell can dispense with more and more of its normal social obligations within a multicellular organism and multiply wildly at the expense of normal cells.
As Duesberg observes, cancerous cells tend to evolve from bad to worse. This process is referred to as carcinogenesis and is characterized by the cells developing their own unique sizes, shapes, metabolisms and growth rates. Malignancy is defined by the cancerous cells' abnormal ability to invade neighboring tissues and to travel to distant organs, a phenomenon known as metastasis. The evolutionary plasticity of cancerous cells is the reason that cancer is an intractible problem, scientifically and medically. Soon after a toxic drug is found to kill tumor cells, those cells that are resistant to the drug will multiply and grow in their place.
Despite their differences, the entire population of malignant cells came from a single unstable mother cell. This clonal origin of cancerous cells is easily seen by tracing unique chromosomal rearrangements that could only have arisen from one source. So the challenge facing scientists is to determine how one normal cell out of trillions in the human body can become so chromosomally and phenotypically unstable that it gives rise to cancer.
To understand this phenomenon, the author's group began to collect and analyze cellular exceptions to the popular gene mutation theory of cancer. This allowed them to identify six main features of cancer that are inexplicable by gene mutation alone but are explained by gross chromosomal changes.
Cancer risk increases with age. Basically, cancer is primarily a disease of old age and is almost completely unknown in the young. This is consistent with chromosomal disturbances hypothesis because gene mutations accumulate over generations. Thus, even though newborns can harbor enough gene mutations to trigger cancer, they rarely have cancer. Additionally, lab mice that are intentionally engineered to carry an assortment of carcinogenic mutations from birth can live and propagate with no higher risk of developing tumors than normal lab mice. So this suggests that something other than simple genetic mutations are the likely cause of cancers.
Also consistent with these observations, and a rare exception to cancer's age bias, are children that suffer from congenital aneuploidy, such as Down's Syndrome, or from an inherited chromosomal instability syndrome, such as mosaic vareigated aneuploidy (MVA), both of which cause mental retardation. These inborn errors result in disturbances to chromosomal structure or number. For example, it is known that defects of the spindle assembly in the cells of MVA children produce random aneuploidies throughout their bodies, and nearly one third develop leukemia or unusual solid cancers. Thus, being born aneuploid or with the propensity towards aneuploidy accelerates the process that leads to cancer.
Carcinogens take a very long time to cause cancer. After exposure to numerous chemicals and forms of radiation that are known to be carcinogeonic, it is known that even the strongest carcinogens at the highest survivable doses do not cause cancer immediately. Instead, cancer only shows up years or decades later. However, when bacteria are exposed to substances that cause gene mutations, they begin to display their new phenotypes within hours, and in larger organisms, such as fruit flies, this effect is seen within days. Thus, the gene mutation scenario does not explain why cells exposed to carcinogens become cancerous.
Carcinogens, whether or not they cause gene mutations, induce aneuploidy. Some of the most potent carcinogens, such as asbestos, tar, aromatic hydrocarbons, nickel, arsenic, lead, plastic and metallic prosthetic implants, particular dyes, urethane and dioxin, do not typically produce any mutations at all. Moreover, the dose required to mutate any one gene can be a thousand times greater than that required to induce malignant tumors years later. But it was noted in all cases that the chromosomes of cells treated with these carcinogens displayed higher than usual rates of breakage and disruption. Thus, carcinogens function as "aneuploidogens" rather than mutagens.
Patterns of aneuploidy are seen in different tumors. If aneuploidy is a side effect of cancer, then chromosomal changes in the cancers of different people should be random. But in fact, based on findings using several chromosome painting technologies, scientists are detecting distinct non-random chromosomal patterns in cancer cell genomes. These technologies allow scientists to tag specific regions of chromosomes with colored DNA-specific probes and to construct pictures of the chromosomal pieces that have been gained, lost of rearranged in each cell. For example, a group at Karolinska University Hospital in Sweden found that patients suffering from Burkitt's lymphoma had translocations involving chromosomes 3, 13 and 17, as well as specific losses or gains in chromosomes 7 and 20.
Additionally, researchers have found that specific chromosomal changes are associated with the particular stage of the cancer, its metastatic potential, and drug resistance. For instance, the Karolinska group found that translocations of a particular region of chromosome 17 and gains on parts of chromosomes 7 and 20 were associated with drug resistance.
Gratuitous traits do not contribute to cancer's survival. Individual gene mutations, which rarely occur, would only be selectively conserved in tumor cells if the mutation gave those cells an advantage. So the chances of an untreated cancer developing resistance to a drug it has never been exposed to before and metastisis, which does not help the cell to successfully compete with normal cells at the site of origin, is practically zero. But because chromosomes contain thousands of genes, they can be selectively retained for their contribution to some cancer-specific phenotype, and many other unselected traits, such as drug resistance and metastic potential, also located on that same chromosome, would tag along. Because of this, cancer cells can evolve all sorts of new and unexpected traits very rapidly.
Cancer cells change much faster than genes. As you might have surmised from the previous point, cancer cells can evolve new phenotypes and lose old ones very rapidly -- much more rapidly than normal gene mutations occur. In fact, the mutation rate for each individual gene remains normal in more than 90 percent of all cancers. Instead, aneuploid cells reshuffle their chromosomes and phenotypes much faster than mutatation can alter their genes. Further, those cells that were more aneuploid were quicker to alter their chromosomes, a pattern that strongly supports the conclusion that chromosomal instability in cancer cells is catalyzed by cellular aneuploidy itself.
These collective observations were summed up nicely by Leslie Foulds of the Royal Cancer Hospital in London: "no two tumors are exactly alike ... even when they originated from the same tissue ... and have been induced experimentally in the same way." This individuality of cancers cannot be explained by the activity/inactivity of specific genes, which would be expected to have consistent effects each time in the each cell.
Instead, by recognizing cancer as a chromosomal rather than a genetic disease, medicine can act accordingly. So once a cancer has been identified, this aneuploid scenario shows how random chromosomal reshuffling can rapidly generate lethal properties such as drug resistance and metastasis. As a result, treatment paradigms that rely on using one drug, for instance, especially those drugs that target one gene, will not be effective. Additionally, this can help in diagnosis: by determining the level of aneuploidy in a given cell population, scientists can detect and distinguish early cancers from morphologically similar benign tumors. Further, in the case of more advanced tumors, identifying the level of aneuploidy can be used to guide treatment choices.
Finally, screening for chromosome-damaging substances in food, drugs and in the environment could significantly improve cancer preventiion by identifying pottential carcinogens. This knowledge will provide a basic understanding of cancer, yielding effective prevention, management and even cures.
Source:
Chromosomal Chaos and Cancer, by Peter Duesberg. Scientific American, May 2007, pp. 115-122.
I'm afraid this sort of theory is not exactly new in the cancer field, indeed variations of its basic hypothesis have been the motivating factor behind a lot of prognostic cytogenetic analysis of malignancies (mainly leukemias) over the past thirty years. Chromosomal analysis has largely been superceded by tiled genomic array studies which reveal much more detail of the genomic alterations within tumor samples. From my own experience I can say that aneuploidy is rather common but in no way essential in tumors. Many tumors appear karyotypically normal by cytogenetic or tiled array analysis yet they behave just as aggressively as those cases with obvious chromosomal alterations.
A much more interesting (IMHO) study is that by Beilas et al in PNAS late last year where they developed an assay that showed that human cancers express a mutator phenotype. In other words cancers have an incredibly high mutation rate. This allows them to generate the variation neccessary to evolve into the malignant disease we have such difficulty treating. Other recent papers by Sjoblom et al in Science and Greenman in Nature have looked at various tumors using massive sequencing strategies, revealing much higher numbers of mutated genes than previously estimated. These major sequencing studies are only coming on line over the past few months and strongly indicate cancer is a genetic disease with a strong heterogeneous clonal evolutionary component.
The paper, "The hallmarks of cancer," by Hanahan and Weinberg,
http://www.weizmann.ac.il/home/fedomany/Bioinfo05/lecture6_Hanahan.pdf
has an interesting interpretation. The six-or-so things that have to go wrong with a population of cells for it to become a full-fledged cancer appear to happen in a well-defined sequence that can be explained in terms of natural selection.
First, a mutation occurs in a cell making it self-sufficient in growth signalling. This can be any of a variety of things: expressing a growth factor to which the cell itself responds, or making variant types of any one of a number of signalling molecules in the MAP kinase pathway.
Now the cell is capable of unlimited mutation, and can grow in a dysplastic fashion. Nevertheless, its growth is still severely limited by contact inhibition and anti-growth signals from neighbouring cells. The population of self-signalling cells is thus under a certain degree of selective pressure to acquire a second mutation, turning off contact inhibition and allowing runaway cell division. Now there is a proliferative colony, and this stage is what a pathologist might call a dysplastic lesion, or an interstitial neoplasia. It's still "benign".
This lesion grows, but eventually it is starved for food and oxygen and poisoned by its own waste products. The lesion degenerates, becoming dormant or even necrotic in the center, with only an indolently growing periphery. Once again, the population of rapidly dividing cells is under tremendous selective pressure to acquire yet another mutation, this time to command angiogenesis so that new vasculature can nourish the tumor. This mutation is usually somthing that results in the upregulation of VEGFA. At this point, a pathologist might refer to the state of the lesion as "carcinoma in situ."
The growth is still limited, though, by cellular senescence and the Hayflick limit. With each round of cell division, the telomere is shortened until the telomere on at least a couple of chromosomes is effectively absent. At this point, aneupliody becomes extremely likely, since the naked ends of the chromosomes splice to one another fairly freely, and then the chromosomes with multiple centromeres are mis-sorted and even ripped apart on the mitotic spindle. The disruption of the DNA, however, activates the DNA proofreading in the cells, and cells with the shortened telomere usually apoptose. This situation gives rise to selective pressure to turn off apoptosis by disabling the G2-M checkpoint, and a population of cells arises with an ineffective variant p53, an inactive pRB, or something related.
At this point, tremendous genomic instability enters the picture, allowing for much more heterogeneity in the lesion and rapid evolution of the cancer. There is selective pressure to at least keep a functioning genome, so cells that mutate to express telomerase are at a tremendous selective advantage - so a population of immortalized cells can arise.
Now there is a full-fledged cancer - the pathologist will see a population of small round blue cells, generally poorly differentiated. The final step, again enforced by selective pressure, is to acquire the ability to degrade the intercellular matrix, invade surrounding tissue, and metastasize.
It appears that these six characteristics (self-sufficiency, disinhibition, angiogenesis, defective apoptosis, immortalization, and invasion) are acquired in a remarkably consistent order, although in any given cancer, there may be a different set of mutations giving rise to these phaenotypes. Aneuploidy appears comparatively late in the progression from borderline dysplasia through a benign lesion, to carcinoma-in-situ, to full-blown invasive cancer.
Here the aneuploidy can be understood both as a mechanism enabling rapid evolution and as an effect of the damage to the telomere that arises before the cell population is immortalized. Without considering evolution and population dynamics, aneuploidy is by itself a poor explamation of the phenomenon of cancer.
Chromosomal instability is certainly a feature of most cancers but I don't think there is any convincing evidence that it is necessarily driven by aneuploidy. Duesberg argues that a single mutation wouldn't be capable of unbalancing the expression of large numbers of genes but that is clearly not true. Plenty of single gene mutations in transcription factors or DNA repair enzymes or cell signalling molecules can alter expression of dozens or hundreds of downstream genes.
Also, aneuploidy is far easier to detect than mutation. All tumors may be aneuploid if one looks closely enough - but all tumors also carry mutations if one looks closely enough. The problem is that assays for mutations can only examine an incredibly small fraction of the total genome at one time and will not detect mutated cells in a background of predominantly normal cells while assays for aneuploidy examine the entire genome and can detect single aneuploid cells in a largely diploid background. It seems obvious to me that if you go looking for aneuploidy and mutation in any cell population, be it cancerous precancerous or normal, you're going to find the former much more easily than the latter.
I'm really confused why this story gets so much traction, because the idea that aneuploidy causes cancer is a very old one (it dates back to around 1914, as a poster at the AACR meeting in L.A., from which I just returned, pointed out ). Duesberg has in essence started acting like he's the one who thought of it. He's also representing it as more controversial than it is. Yes, it's a somewhat controversial, but no more so than the hypothesis that metabolic derangments (i.e., the Warburg effect) are a major cause of cancer. If it weren't for Duesberg's HIV/AIDS crankery, he wouldn't be causing any waves. I also can't help but point out a couple of things: First, there was a very fascinating talk at the AACR about how metabolic derangements can lead to the production of reactive oxygen species and ultimately lead to chromosomal breaks and aneuploidy; so again, the chicken-or-the-egg problem comes up. Second, John Neiderhuber, the Director of the NIH, gave a talk in which he outlined the five or six priorities for research at the NCI. Obviously cancer stem cells were one area. But one area was the idea that derangements in the 3D arrangements of chromosomes are a major contributing factor in cancer, a hypothesis Dr. Neiderhuber called one of the most "fascinating" ideas he's seen in years.
In any case, the whole thing is a "chicken-or-egg" problem? Do gene mutations occur first and lead to chromosomal rearrangments, or is it the other way around? Do metabolic derangements (the Warburg effect) lead to the chromosomal rearrangements? Chromosomal instability is a hallmark of cancer, but Duesberg has not made the case that it's the primary cause, not by a long shot. Chromosomal chaos could easily be a secondary phenomenon. Indeed, it probably is for most cancers, although it's possible that it's a primary cause in some. Remember, cancer is not just one disease, but hundreds of different diseases.
As for using aneuploidy to guide prognosis, jumpin' Jesus on a pogo stick! There are many, many papers out there that look at using chromosomal abnormalities for prognosis. Just do a PubMed research for "translocation," "chromosome," and "cancer," if you don't believe me. It's obvious that Duesberg is no clinician, or he would already know that this sort of prognostic assay has a checkered past and has produced very few useful tests, all of which are based on the presence of a specific translocation for a specific cancer. As for using it to guide targeted treatment, it's of limited applicability; only when a specific translocation leads to the overexpression of specific oncogene is targeted therapy useful. One example is a reciprocal translocation between chromosomes 9 and 22 and cytogenetically evident as the Philadelphia chromosome in chronic myelogenous leukemia. This activates the Bcr-Abl oncogene, which can be treated quite effectively with Gleevec.
Damn. Now I'm probably going to have to read this article over the weekend and perhaps blog about it.
when i was working in cancer research, i was aware of this hypothesis as well, although i was not sure who was the original architect of it. anyway, i summarized this article because i don't think that the public was generally aware of it.
Duesberg has in essence started acting like he's the one who thought of it.
I also read Bialy whining that a recent review did not cite any of Duesberg's work so it seems that Duesberg's claim to be behind the recent work in the field is also exaggerated.
Perhaps Duesberg should also repeat his HIV/AIDS mantra "correlation doesn't equal causation" a few more times.
Some such as Orac and Chris Noble and others still would like to pretend that Duesbergs work in cancer is to be ignored. They contend that Peter must be trashed and all his good works are simply not so. To hell with unraveling cancer or AIDS, they must protect the stand they have taken! They, and multitudes of others who bought the bull that HIV causes AIDS are all very threatened by anything Dr. Duesberg says or does, such as the responses to this current piece on aneuploidy clearly shows!
Go for it kiddies. Show us just what you are made of.
For those not in the know, it turned out that the supposed discoverer of HIV; Bob Gallo's retroviral sample of what Gallo called HTLV-III, but was then called LAV by the french lab that actually isolated it, WAS STOLEN from the French lab of Luc Montagnier, most likely because Gallo and the American team was terrified that the French had solved why drug and sex addicted gays got immune dysfunction called AIDS, and they were terrified that someone would find a virus that was causing AIDS before the Americans did.
At a press conference on the White House steps of then president Ronald Reagan, with secretary of health Margaret Heckler at his side, on April 20th 1984, Robert Gallo held a press conference and proceeded to DECLARE to the world press that HIV was the cause of AIDS weeks before he even published his results, and years before anyone else could or would confirm or dismiss the claim. This egoically driven haughtiness is, was, and always will be, fraudulent science. This is wrong! And also quite wrong is the deceitful continuation of it, in the form of science by popular opinion, which has kept Peter Duesbergs work on HIV in the dark for 20 years, and his work on Cancer in the dark for 25 years.
And, this science by fraudulent press declaration was not even the first fraudulent and questionable thing that National Cancer virologist Robert Gallo had done. He had attempted to do the very same thing a few years earlier with his claim that another retrovirus caused cancer, but not all of his colleagues bought it at the time and he was left with his tail between his legs. But he did pull it off with his HTLV of which he kept his pseudoscientific evidences out of the hands of colleagues who might discredit him, as he worked the higer-ups, such as Margaret Heckler and the director of the NIH into believing him and siding with him.
Nor would this be the last bit of Gallo's fraud. Gallo also patented his HIV test the very same day, for which he has gained 100 thou a year for 20 years! The French immediately sued, Reagan and the French president sat down, agreed not to make American scientists look like thieving idiots, and they agreed to "share" the discovery. Gallo was later found guilty of scientific misconduct in 1993, but all who were by now cashing in on HIV funding all rushed to cover it up and pretend that Gallo's fraud was not so. Sick gays and blacks be damned, they needed to protect the government and their own financing. This fraud yet continues to this day, as now, everyone who did not sceptically look into it for themselves, or bought into the belief before they did look into it, is egoically and emotionally trapped into continuing to promote Gallo's fraud.
It is understandable that all involved at the time rushed early on to cover it up and work like dogs to convince themselves and the public that Gallo was innocent and correct about HIV. What would any of you have done if you were president or surgeon general or head of the CDC or NIH and another leading scientist stands up 3 years and 10 billion tax dollars later and says you have gotten it wrong? Gotten it wrong 3 years later after hundreds of scientists, billions of dollars, and millions of people think you knew what you were doing? If you think government coverups such as no WMD's in Iraq is a problem today, just think of how it was for the government officials 20 years ago when the public was paralyzed by the paranoia that the modern black plague of AIDS was descending upon them! Many still live in terror of a modern plague of Sars or Bird Flu!
Interesting that in the SA article, the editor felt the need to pacify the fears of the faithfully paranoid advocates of HIV with his editorial saying Duesberg was thoroughly rebutted about HIV.
Peter Duesberg was never rebutted. He was and still is out and out rejected by the same virologist pigs feeding at the taxpayer paid HIV trough, just as they are yet doing by feeding on the public paranoia of Sars and Bird flu. And let's also pay homage to the other paranoid pigs feeding on the pharma companies trough, as if magic pills and vaccines will ward off the evils of the plague that must come. And let us all pay homage to the yet brainwashed masses and followers who follow these scientists as if HIV and Sars and Bird Flu were a religion that only the deranged would disagree with.
By the way, even Robert Gallo said in the Supreme Court testimony in an HIV trial in Australia 3 weeks ago, that 99 percent of the HIV "experts" came from the failed and now closed cancer-virus program. These guys were desperate to rally around something to save their jobs, and Gallo provided the solution. Duesberg threatened it and had to be sacrificed for the good of the many ( of the many virologists, not the good of the now paranoid and scared sick public masses of gays, druggies, blacks, and poverty stricken, who are 99.99% of the affected, and easily explained by other factors).
The only lesson to learn from what happened to Peter with HIV and his cancer research, is DO NOT get in the way of the feeding frenzies of pigs, nor of the brainwashed and paranoid and delusional masses!
Duesberg was cast out and sacrificed, most likely subconsciously, to save the scientific finances and to save the paranoid egos, as well as to save the White House of Ronald Reagan, where Gallo had his press conference wherein he "declared" he found the cause of AIDS way back in 84. The others who would have had the most to lose at the time and still do, were the other scientists who unquestioningly and unsceptically followed and still do, as well as the heads of the NIH, CDC, HHS, and even the surgeon general. None could stand to have been shown to be fooled by Gallo. Duesberg had to go to save all of their reputations and jobs. Even the gays refused to believe that their popper sniffing, std infested, overly antibiotically treated lifestyles were unhealthy. Understandable, as no one likes to be told they are screwing up.
And many of the fools that think Duesberg has been answered are simply confirming how easy it is to brainwash the unthinking and virally paranoid masses.
Where is the rebuttal to Peter on HIV? By who and when? And please don't tell us it is scattered about somewhere in the mountain of "overwhelming evidence" of 200,000 HIV studies done by the feeding pigs!
Let's look even at Scientific American in an article on HIV 14 long years ago, in explaining the ongoing morass and dilemma of HIV from which nothing has yet changed:
As Warner C. Greene, a professor of medicine at the University of California, San Francisco, explained in the September 1993 Scientific American, researchers are increasingly abandoning the direct cell-killing theory because HIV does not infect enough cells: "Even in patients in the late stages of HIV infection with very low blood T4 cell counts, the proportion of those cells that are producing HIV is tiny-about one in 40. In the early stages of chronic infection, fewer than one in 10,000 T4 cells in blood are doing so. If the virus were killing the cells just by directly infecting them, it would almost certainly have to infect a much larger fraction at any one time."
Peter Duesberg takes no goverment or pharma funding and has not done so in 20 years. He is also the only scientist in America who was willing to sacrifice eating at the pig trough to stand up for the science that he believes in.
Of course, it takes someone with honesty and integrity to see the honesty and integrity of others, therefore I can understand why some of the posters here are unable to see this integrity even if it smacked them in the head with a 2X4! They are yet still far too trapped by the nonintegrous delusions of their own continuing fear and paranoia and egoic positionality to see the forest from the trees!
GS, now that you have attracted those so unfortunate as to believe that AIDS has nothing to do with HIV, as well those who are upset with Duesberg because his statements about AIDS are clearly connected with people dying of AIDS, your blog will be more popular.
llewelly, perhaps you will show us the proof that HIV causes AIDS.
You claim people die of "AIDS" caused by HIV? No one has ever died or ever dies of AIDS. AIDS is a syndrome of failure to recover from any of 30 common illnesses. They die of actual diseases, not of AIDS. OR they die of the toxic drug side effects which are conveniently labeled "complications of AIDS" to keep the pharma companies and prescribing doctors and insurance companies etc, quite safe!
AIDS is simply a diagnosis given to anyone with any of these 30 common diseases who also happens to have tested HIV positive, or given to someone who is perfectly healthy and has low CD4 counts. Recent papers proved that CD4 counts only reflect who becomes ill in less than 5 percent of HIV cases!
Would you claim that all AIDS cases have HIV? Well, if so, of course you are right because if someone is HIV negative, any disease they get is called and diagnosed as its common name such as herpes, pneumonia, tuberculosis, ovarian cancer. Only when someone is HIV positive and comes down with any of these is it called "AIDS".
All of the risk groups, from gay men who have intense emotional problems and sex and drug addiction and antibiotics overuse from exposure to many std's, to the hemophiliacs of 20 years ago who were exposed to now banned blood products, to the starving and poverty stricken of 3rd world countries have COMPLETELY DIFFERENT DISEASES AND SYMPTOMS, all of which are easily explainable by other causes than HIV.
Would you hide behind twisted words that have obscured meanings? Would you claim truth as lies and claim lies as truth. The world is waking up to the fraud of HIV and AIDS!
Furthermore, telling someone that they have an incurable virus leads to panicked fear, which alone, over time, leads to immune system failure. How dare you apply your voodoo diagnoses of HIV to scare people sick and then say "I told you that you would get sick". If you would, than You are the sickest of all. You and the rest of the promoters of scaring people to death! And perhaps you believe in promoting the very toxic drugs that cause immune failure, lypodystrophy, liver failure and cancer. Are you for some reason unaware that liver failure is the leading cause of death in HIV positive Americans for the last 10 years?
Come come llewelly. Please do explain all of this HIV and Cancer crap better than Dr. Duesberg, and surely we will elect YOU for a Nobel prize! (you did note that none of the HIV researchers has ever gotten a Nobel prize from HIV research, did you never wonder why)? OR snap out of your obviously meme infected brain and wake up and look for yourself at the research and at the unanswerable questions that Peter Duesberg and thousands of others are asking!
Why is HIV never found in the T cells it supposedly kills? Why is there never enough evidence of HIV in enough cells to cause any damage? Why is their always other usually simple explanations than HIV easily available for all supposed AIDS cases?
And hey grrlscientist.
I for one greatly appreciate your bringing Peter's important work on aneuploidy to light without the usual condemnation of anything that comes from Peter Duesberg must be wrong. Are they all really so sure about HIV causing immune suppression when after 25 years, so little of it makes sense, or are they brainwashed by the foolish paranoid virologists of the cancer institute turned HIV experts that Peter used to work with at the NCI and is quite glad to be free of for the last 20 years.
Are virologists mostly a bunch of delusional paranoids? Take a look at Sars and Bird Flu, and you tell me!
"Some such as Orac and Chris Noble and others still would like to pretend that Duesbergs work in cancer is to be ignored"
Bullshit. My point is that Duesberg's work in cancer is not nearly as revolutionary or controversial as it is painted by his sycophants.
um, thanks, i think, except you have me all wrong when it comes to HIV and AIDS. i did write this summary piece for my readers to enjoy, especially those who do not have a subscription to SciAm -- i trust that they can judge for themselves what to think of it without my opinions.
but i will point out that, in addition to working in cancer research for several years, this molecular-evolutionary-ornithologist-type also worked with HIV for a couple years and basically, the evidence shows that HIV causes AIDS. Duesberg is plain old wrong with regards to HIV.
bird flu and SARS are two other topics that i haven't written much about recently, although i probably should, and probably will in the future.
Thank You, GrrlScientist, for making this topic easy for a laymen as myself to understand! I luv this stuff and you work the "info." so well. :o)
Thanks for the response GrrlSci. But one of the simplist points, which is not anything about Duesberg, is the following?
What is the effect on someone's physical health, of telling them that they are infected, due to their sexual behaviors with a virus that will slowly kill them?
Are you completely unaware of the effects of emotions and beliefs on health?
What kind of medicine practice is it to take away someones hope to live by telling someone that they are doomed to die a slow death from any of 30 or more common diseases?
Surely you are capable of empathizing with others a bit, I would hope. So will you consider the following? Lets start with the following supposition, which of course is not true, but if it were, how would you "feel"? If first off, you are not very attractive, were never good at sports, or never felt any part of the "in crowd". In other words, you never felt as if you were ever good enough. Now add to this that you are also a homosexual. Are you capable of empathizing with someone who already often feels like a social leper due to the difference in sexual preference from what 90 some percent of the population considers to be acceptable and "morally OK", and now add to this that you are suddenly told that you have HIV and it is incurable.
Are you aware that to a sexually active person, this is pretty much just like being told that you now are a complete sexual leper as well as already seeing yourself as a social leper, who will most likely kill anyone that you have sex with if any of your deadly filthy and infected and contaminated body fluids should ever come in contact with another human being?
Please tell me grrl, how you would feel if this were to be your lot in life? How do you suppose it would affect your physical and emotional health, particularly if you are already under the stress of your own self rejection and your own lack of self acceptance of your own sexuality. Particularly if you knew that even your own parents would be filled with shame, loathing and disappointment and complete rejection of you if they ever found out that you were a social misfit of a homosexual. Particularly if even your own parents disowned you for being gay and told you never ever to call them again. And particularly if you could not even go to the pastor of your childhood because he teaches that being a homosexual is an abomination to God.
Might you not, just from the stress alone, even perhaps wish at times that you were dead? Might you not feel as if you were a mistake that never should have been born? Might you not feel unworthy of love and life? Might you not even feel quite hopeless and helpless, and perhaps wish to end your life sooner than later?
What is the impact of such thoughts and emotions on ones physical well being? Please tell me your thoughts on these quite real realities for many people that you most likely have never even remotely considered grrllscientist.
Would it not also be a temptation for many, with going through such emotional difficulty as this, to drown your emotions in drug or sex abuse to escape the difficult and painful emotions? Would the effects of drug abuse and the effects of antibiotics overuse due to continuous exposures to std's and std treatments be beneficial or detrimental to your health?
I have known many whose pathetic lives and pathetic emotions are exactly what I have just portrayed to you. They are now dead, and it was called AIDS.
And you, grrlscientist, think you can simply blame the ensuing inability to recover from pneumonia or from anything else you happen to come down with on a measely 9kb retrovirus that cannot even replicate without becoming an integral part of your DNA, that has never been found in amounts that could do any damage even in patients supposedly dying from it, that has never been isolated from human t cells?
What kind of medicine practice is it to take away someones hope to live?
Can you say VOODOO MEDICINE???
Wow, you all are a bunch of bickering kids. I disagree with Duesberg and think his analysis of HIV's causation of AIDS is rediculous. HIV causes AIDS. But fortunately, after years of cancer research I have figured out that HIV/AIDS and cancer are two different issues. So, let me say that I am perfectly willing to hear Duesberg out and found his article very interesting. Thank you to GrrlScientist for summarizing it. We need more scientists to translate scientific articles into lay writing so the public can be more informed. So my humblest thanks to you. For those of you out there who are skewing this blog debate to indict those critics of Duesberg's AIDS views and not listening to what they are saying about cancer, I say shame on you. We are generally supposed to be scientific proponents, so get your clouded minds out of this blog and try discussing the cancer. As for the article, let me say the following. My research focuses mainly on the pharmacogenomic value of single nucleotide polymorphisms. For the non-scientist out there, that means that I look to see what mutations in a patient's DNA are linked to certain side effects from the various cancer drugs. Therefore, and through other research in the lab, I have seen the effect of the genetic mutation theory of cancer. That and Knudson's two hit hypothesis (a theory that in essence says that a certain number of "hits," or genetic mutations are the predisposers for cancer) are pretty good evidence that you cannot ignore polymorphic mutations in such a haphazard manner as did Duesberg. That is not to say that they are the only cause of cancer. I agree with Orac that we cannot be sure about which comes first. The lab I work at has done aneuploidy analysis and copy number analysis to see if those chromosomal anomalies are pharmacogenomically predictive. However, while reading the article, I think that Duesberg, as a scientist, made a fatal flaw. I cannot accept in good faith that we must dismiss the genetic mutation theory of cancer and just accept Boveri's (and now apparently Duesberg's) chromosomal aneuploidy theory. I like to think of this like the recent diet fads. There is no one way to get rid of all that excess fat. Everything in moderation. Perhaps it is not just chromosomal anomalies, genetic mutations, or the metabolic effects of the Warburg theory that are the sole cause of cancer. Perhaps, everything in moderation is the way to go. I think Orac was the first in these series of posts to dig into this. Perhaps, and I have no answers and think only time will tell, we will find out that chromosomal rearrangements AND genetic mutations work in conjunction to exacerbate the problems faced by a cell that will eventually become malignant. That the mutations drive chromosomal rearrangement and chromosomal rearrangement drives genetic mutations may ultimately be the solution to the "big picture" that Duesberg claims to be able to see with his work. So in conclusion, I do not think cancer has a single cause. It was pointed out that there are 100s of types of cancer and we know that every human is unique; therefore, I would suspect that no one cause cancer will be found, but in the words of my physics friends, perhaps there is a unifying theory of what causes cancer that can put the genetic mutation camp on peaceful terms with the Duesberg/chromosomal rearrangement camp.
thanks for your comments, JAS. i summarized the article because i was interested to explain this hypothesis for cancer to my readers. i probablky should have been more opinionated about this article because i disagree with Duesberg's HIV-doesn't-cause-AIDS rubbish and i also disagree with Deusberg that chromosomal rearangement is the only trigger for cancer (i worked with HIV and with p53 in cancer research, so i am well aware that there are other causes for cancer). however, i wanted to present this info to the public (who might not have a subscription to SciAm) to further their understanding of cancer as well as giving them a forum for debate.
To GrrlScientist: This whole topic is new to me, being one of the uneducated public who just read the SA article on Chromosomal Chaos. As an additional question, I also just read somewhere that p53 in an active form might be a cancer promoter and that where drug treatment is successful, p53 is deactivated. Can you commment on that at this time?
actually, i worked with p53 as an undergrad. p53 is a tumor supressor gene that, when it becomes mutated, allows solid tumors to grow. if p53 remains unaltered, it does its job properly and prevents solid tumors from growing.
and yes, Duesberg is incorrect in asserting that only chormosomal chaos causes cancer -- there are plenty of small mutations, even some point mutations, that lead to cancer. when i was working in cancer research, i came to the conclusion that there are nearly as many causes for cancer as there are cancers themselves.