
One of the most effective spin techniques used by advocates of “integrative medicine” (also sometimes called “complementary and alternative medicine,” or CAM for short) to legitimize quackery has been to claim basically all non-pharmacologic, non-surgical interventions as “integrative,” “complementary,” or “alternative.” Thus, science-based interventions such as diet changes to treat and/or prevent disease, exercise, and other lifestyle alterations are portrayed as somehow so special, so outside the mainstream, that they need their own specialty, “integrative medicine,” even though they are simply part of medicine. I pointed this out a mere two weeks ago when I discussed the National Center for Complementary and Integrative Health (NCCIH) review of non-pharmacological treatments for pain. It was a systematic review that was essentially negative but spun as positive for some interventions and lacked some key analyses that a good systematic review includes, such as assessment of the quality of the studies included and evaluating them for bias.
Such were my thoughts as I encountered an article from the American Society of Clinical Oncology (ASCO) that came up in e-mail lists. The article discussed the actual evidence for the utility of diet and exercise for cancer prevention. It’s almost as though Twitter were telling me it was time for me to discuss this issue from a science-based perspective. So, taking the hint, I will attempt to do so.
Diet and exercise versus cancer: The evidence
A couple of weeks ago, I saw in my e-mail in box this article, Impact of Adherence to Cancer Prevention Guidelines on Diet, Physical Activity on Cancer Risk and Mortality (PDF). My first thought when reading this summary was that this is cool, something I need to read. My second thought was, given my recent Twitter exchange now would be a good time to blog about it. My third thought, which came as I went searching for the actual study, is why it took ASCO two months to feature the story, given that the actual study by Lindsay N. Kohler, MPH and co-authors had been published in July in Cancer Epidemiology, Biomarkers & Prevention. I also noted that it came from the University of Arizona, which did raise red flags for me given that that is the home of the godfather of “integrative medicine,” Andrew Weil, but fortunately the systematic review came out of the Department of Nutritional Sciences and the Mel and Enid Zuckerman College of Public Health. That’s not to say that I wasn’t concerned somewhat, given that the Zuckerman College of Public Health made a deal last year with Southwest College of Naturopathic Medicine to offer a dual-degree program for a naturopathic medical degree (ND) and a master’s degree in public health (MPH), slated to begin this term.
Still, I decided to take a look at the review on its merits. It begins with a discussion of existing dietary and exercise guidelines for health and cancer prevention developed by the U.S. Department of Health and Human Services along with health organizations such as the American Cancer Society and the World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR). These cancer prevention and health promotion guidelines focus on specific lifestyle recommendations to
- Achieve and maintain a healthy weight throughout life
- Adopt a physically active lifestyle
- Consume a healthy diet with an emphasis on plant-based foods
- Limit alcohol consumption
Looking at the detailed ACS guidelines (lay version here) originally published in 2012 and the WCRF/AICR guidelines, I realize that I’m probably not doing so great. Granted, I recently started a concerted effort to alter my diet and lose about 20-25 lbs, which would bring me back to a pretty healthy weight, and to exercise by bicycling several miles five or more times a week, taking more brisk walks, and taking the stairs instead of the elevator more often, but I still am sedentary a lot and really have a hard time sticking to the more plant-based diet. In this, I rather suspect that I’m not unlike a lot of middle-aged guys whose jobs don’t involve physical labor.
My own personal difficulties grappling with trying to adopt a healthier lifestyle aside, Kohler et al sought to determine whether adherence to the ACS guidelines is associated with a decreased risk of cancer. In other words, do the guidelines work? To this end, they undertook a systematic review of the epidemiology literature, focusing only on prospective cohort studies. That means that the investigators followed the subjects in their cohorts only after they were enrolled in the study. Prospective studies are generally considered a higher level of evidence than retrospective studies (studies that look at patients in the past) because recall bias can be decreased, objective measurements can be taken in a standardized fashion, and the effect of confounders can be decreased. Here’s how the studies were chosen:
Only prospective cohort studies were eligible for inclusion, as the focus was to ascertain cancer incidence and cancer mortality. Minimally, studies must have collected data for physical activity and diet, generated an adherence score on the basis of either ACS or WCRF/AICR cancer prevention guidelines (2, 12), and reported cancer outcomes of incidence and/or mortality to be deemed eligible for this review. Overall cancer incidence and cancer mortality were the primary outcomes of interest. However, site-specific cancer risks were also considered when data were available from at least two studies meeting the eligibility criteria. Commentaries and summary documents were excluded unless they presented additional data.
Resulting in the following studies being chosen from the database databases the current recommendations of Preferred Reporting Items for Systematic Reviews and Meta-analysis Approach (PRISMA):
A total of 2,033 potentially relevant studies were reviewed; after removal of duplicates and exclusion on the basis of title or abstract, 25 full articles on nutrition and physical activity cancer prevention guideline adherence were retained for in-depth consideration. The selection process for the articles is shown in Fig. 1. We identified 12 articles that met the a priori criteria for inclusion (Table 1). These studies represented analyses of data from 10 cohorts including the Cancer Prevention Study-II (CPS-II) nutrition cohort (13), the Women's Health Initiative (WHI) cohort (14), the NIH-American Association of Retired Persons (NIH-AARP) Diet and Health Study cohort (15), the Framingham Offspring (FOS) cohort (16), the Vitamins and Lifestyle (VITAL) Study cohort (17), the Canadian National Breast Screening Study (CNBSS; ref. 18), the Swedish Mammography Cohort (SMC; ref. 19), the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort (20, 21), the Southern Community Cohort Study (SCCS; ref. 22), and the Iowa Women's Health Study (IWHS) cohort (23).
Reviewing the 12 studies, Kohler et al found that high adherence to established nutrition and exercise guidelines was associated with decreases of 10% to 61% overall cancer incidence and mortality. The study finding the greatest reduction in risk was the analysis of the VITAL study by Hastert and colleagues, which found that meeting at least five recommendations from the WCRF/AICR guidelines compared with meeting none demonstrated a 61% reduction in cancer-specific mortality over 7.7 years of follow-up (HR, 0.39; 95% CI, 0.24–0.62). The study that showed the lowest decrease was a study utilizing the ACS guidelines including nearly a half a million men and women aged 50-71 years in the NIH-AARP Diet and Health Study. Basically, Kabat and colleagues reported a statistically significant decrease in cancer incidence over the 10.5 years of follow-up for both highly adherent men (HR, 0.90; 95% CI, 0.87–0.93) and women (HR, 0.81; 95% CI, 0.77–0.84). A statistically significant reduction in cancer mortality was also reported during the 12.6 years of follow-up for both highly adherent men (HR, 0.75; 95% CI, 0.70–0.80) and women (HR, 0.76; 95% CI, 0.70–0.83; ref. 27). In fact, here’s a table summarizing the studies (click to embiggen, if necessary):
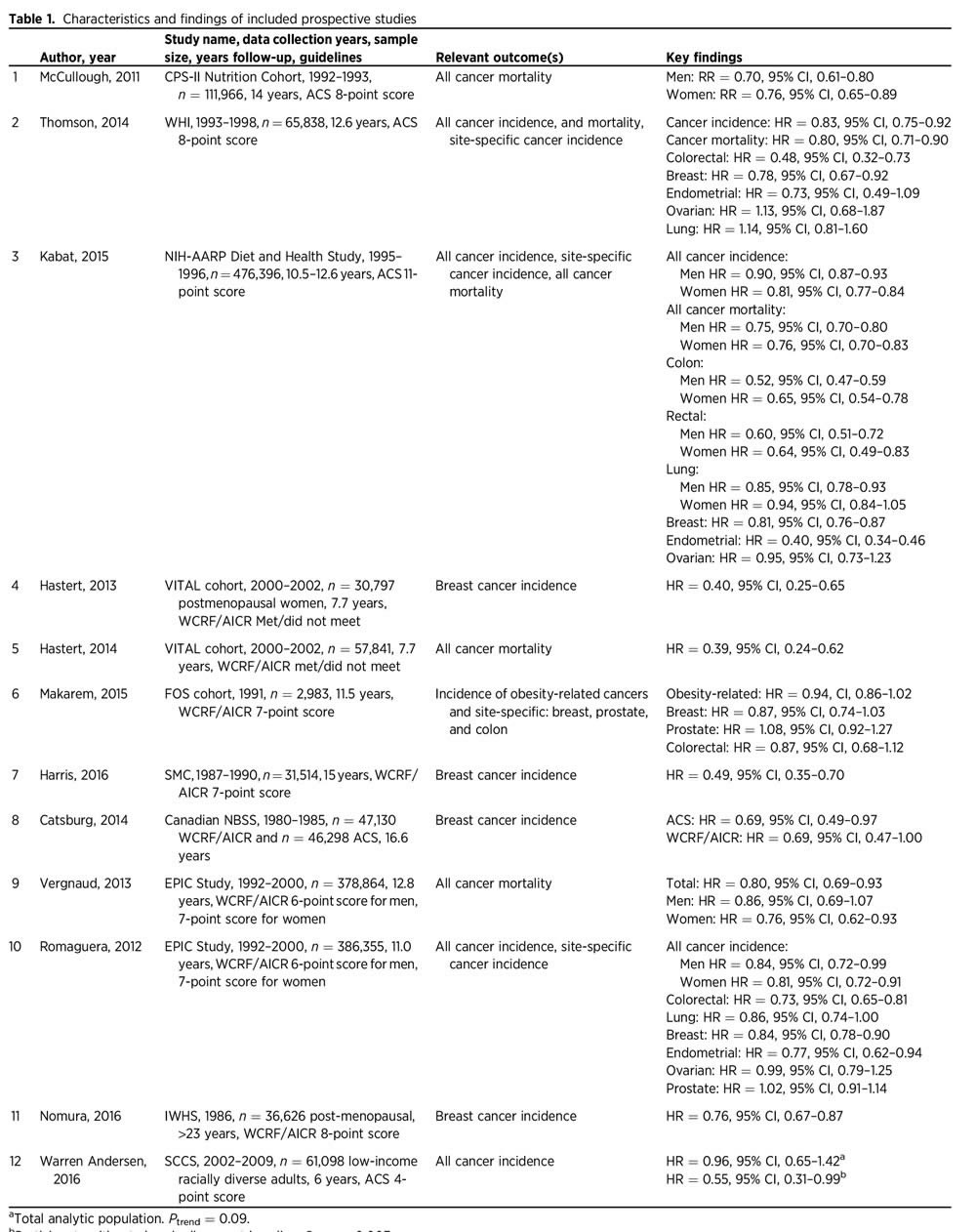 Diet and exercise vs. cancer: A summary of the evidence.
Diet and exercise vs. cancer: A summary of the evidence.
Yes, the figures are all over the place, but there is a consistent association with adherence to the ACS or WCRF/AICR dietary guidelines with decreased overall incidence of and mortality from cancer. The variability can likely be explained by the differences in the cohorts (for instance, the NIH-AARP cohort consisted only of people over 50, an age when people enter the most cancer-prone period in their lives), how adherence scores were defined, and the like. But what about the effect of diet and exercise on individual cancers?
Diet and exercise versus individual cancers
The authors also looked at the effect of adherence to these diet and exercise recommendations on the incidence and risk of mortality from individual cancers, primarily breast, colorectal, lung, and endometrial cancer, because these are the cancers for which the most studies were available.
For breast cancer, there were eight studies reporting results for breast cancer. Kohler et al note that there were consistent reductions in breast cancer incidence reported in the WHI, NIH-AARP, and EPIC cohorts for high adherence to nutrition and physical activity cancer prevention guidelines versus low adherence, for a reduction in risk. Also, meeting at least five WCRF/AICR recommendations compared with meeting none was associated with a 60% reduction in breast cancer incidence. Overall, the reduction in risk associated with high adherence to guidelines compared to low adherence ranged from 19%–60%, although one of the studies did not reach statistical significance.
Results were similar, although there were fewer studies, for colorectal cancer and endometrial cancer. Basically four of these studies reported results for colorectal cancer specifically, with decreased risk of this disease found in the WHI cohort and the NIH-AARP cohort, as well as the EPIC cohort. The FOS cohort showed a trend towards decreased risk of colorectal cancer that did not reach statistical significance. Taken together, the four studies suggested a reduction in risk associated with adherence to diet and exercise guidelines ranging from 27%–52%. In the case of endometrial cancer, there were three studies that examined this cancer as an endpoint. Both the NIH-AARP and EPIC cohorts both found decreased risk associated with higher adherence to guidelines, and, again, there was one cohort (WHI) with a finding of decreased risk that did not reach statistical significance; the overall decrease in risk reported was 23%–60%.
Finally, the authors examined lung cancer. Of course, lung cancer is unique in that it is a cancer for which the main lifestyle cause is unequivocally known: smoking tobacco products. Although Kohler et al characterize the effect of adherence to diet and exercise guidelines on lung cancer risk as “equivocal,” my reading of the studies they report leads me to believe that adherence to the diet and exercise probably has little or no effect on the risk of lung cancer. This is not particularly surprising given how powerful the effect of smoking is on lung cancer risk and how uncommon lung cancer not associated with smoking is.
What did surprise me is that there was no association with prostate cancer incidence noted utilizing the ACS guidelines in the NIH-AARP cohort or the WCRF/AICR guidelines in the EPIC or FOS cohorts given that prostate cancer is one cancer commonly invoked as being preventable by diet. On the other hand, the diets touted for preventing prostate cancer are more extreme than those encompassed by the ACS and WCRF/AICR guidelines because they are usually vegan. The authors also found no reduction in risk associated with high adherence to diet and exercise guidelines versus low adherence for ovarian cancer.
Diet and exercise versus cancer: Putting it all together
Physicians have sought to identify modifiable risk factors for cancer for a very long time now, possibly as far back as Hippocrates. Of course, two such factors that rapidly rise to the top of any list for just about any disease must be diet and exercise, and, contrary to the frequent criticism of “conventional” medicine by those advocating “integrative” approaches, a great deal of research has been done examining the effects of various diets, exercise, and the like on the risk of cancer in general and of specific cancers. Unlike the case of drug therapies and other discrete treatments, it’s a lot harder to tease out the effects of diet and exercise on cancer risk because such studies take a lot of subjects (one of those cohorts has half a million subjects) and, because the most common cancers are generally diseases of aging, a long period of time. Moreover, while it’s possible to do a randomized controlled trial for many interventions, the complexities of diet make studying the effects of nutrition in such a manner very difficult. That’s not to say that it can’t be done. Indeed, it is being done, but the same problem exists: Lots of patients and lots of time are still required, which has led some to question whether RCTs are superior to prospective cohort studies for such interventions. The point, of course, is that physicians and scientists, contrary to the stereotype, have not been “ignoring” the role of diet in diseases like cancer. Quite the contrary.
This particular systematic review is touted as the first to examine dietary and physical activity cancer prevention guidelines and aggregate the effects on cancer outcomes reported by the existing scientific literature. As such, the authors note its strengths and weaknesses, which are worth quoting at length:
Strengths of this systematic review include strict inclusion criteria to include only prospective studies that constructed adherence scores to the established cancer prevention guidelines by ACS or WCRF/AICR. All of the studies contained sizeable cohorts with multiple years of follow-up leading to sufficient sample sizes, ample power to detect associations, and sufficient number of outcomes, enabling them to evaluate associations for some site-specific cancers. However, there are also some limitations that must be considered. First, all studies generated their own adherence scores on the basis of recommendations from either the ACS or WCRF/AICR. Most studies assigned points for meeting or partially meeting recommendations, whereas others categorized adherence as “met” or “did not meet” recommendations. Including multiple levels of exposure may better capture the degree of adherence to the guidelines. Although ACS and WCRF/AICR guidelines are very similar, interpretations of how to measure the recommendations varied. Notably, physical activity was assessed several ways including in metabolic equivalents, times per week, and even a physical activity index. Furthermore, studies utilized frequency questionnaires to capture diet and physical activity data. These self-reported measures are well-known sources of measurement error, which may bias findings toward the null, lending to conservative findings in this review. Components of the adherence score were measured singularly at baseline and used to assess cancer risk over time. Repeated measurements of diet and physical activity may have provided an improved exposure assessment of long-term behavior and risk over time. Follow-up times ranged from 7.7 to 14 years, which may not be sufficient for assessing the protective role of adherence to nutrition and physical activity cancer prevention guidelines. In addition, although the studies evaluated large cohorts, there was limited population heterogeneity with regard to race or ethnicity, with the exception of the WHI and SCCS studies. Furthermore, analyses varied somewhat among the studies. All studies evaluating associations with ACS guideline adherence made comparisons of high versus low adherence. One study used WCRF/AICR guidelines to compare “met” versus “did not meet” recommendations (29), whereas a single study evaluated adherence to WCRF/AICR guidelines on the basis of point increments of the overall score (36). Finally, the potential for publication bias is always of concern. Studies with significant findings are more likely to be published than those with null or unimportant findings. Grey literature was included in the search via Google Scholar in an attempt to capture any work that hasn't been formally published (abstracts, conference proceedings, etc.). Even though the studies differed in some measurements of individual score components, construction of the adherence score, specifics of the set of guidelines used, and analytic methods, it is important to note that studies generally demonstrated agreement in their findings even across countries with varying diet and physical activity patterns.
You get the idea. The studies chosen were generally of high quality, but their methodologies for assessing adherence to the ACS and WCRF/AICR guidelines varied considerably. In actuality, to me the very fact that studies of such disparate groups using differing methods of assessment are all finding more or less the same thing tells me that the assessment by Kohler et al is likely pretty robust.
Another thing that has to be considered. This is a systematic review of a very specific question: Does adherence to the ACS and/or WCRF/AICR guidelines for diet and exercise (which, when you come down to it, are strongly similar) decrease the risk of being diagnosed with cancer and ultimately dying of cancer? The answer is yes, and we know at least some of the cancers affected: breast, colorectal, and endometrial cancers. We also know cancers for which adherence to these guidelines probably has little effect: lung, prostate, and ovarian cancers. Of course, this is a very limited number of the cancers that afflict human beings. It’s quite likely that diet and exercise impact the risk of many other cancers. However, this review doesn’t really address the effects of specific dietary and exercise interventions. It doesn’t, for instance, tell us if this food or that food, this nutrient or that nutrient, is associated with increased or decreased cancer risk. Those are different questions, and they are actually questions better suited to RCTs than the question that Kohler et al examined.
The reason proponents of integrative medicine claim so many non-surgical, non-pharmacological interventions is because, although inflated claims are often made for them, they can actually work, in contrast to the pseudoscientific treatments also “integrated” into medicine, such as acupuncture, traditional Chinese medicine (TCM), and the like. There’s a reason why we at SBM have at various times referred to diet, exercise, and other science-based lifestyle interventions co-opted by integrative medicine as a “Trojan horse,” particularly in academia. Once academia brings the nice, shiny “horse” of “non-pharmacological interventions” into its citadel, out jump the Greeks of quackery.None of this, however, means that diet and exercise aren’t powerful tools to promote health. Rather, it’s that they are and should remain part of science-based medicine, rather than being tainted by association with the quackery of integrative medicine. And there is a lot of science out there to support the important role of diet as a modulator of cancer risk.
Unfortunately, taking all the evidence together for individual foods, nutrients, exercise, and diet becomes devilishly complicated and contradictory, too. For example, do you remember John Ioannidis’ systematic review of existing scientific evidence associating specific foods with cancer? I do, as Steve Novella and I both blogged about it. Basically, Ioannidis examined 50 common ingredients at random out of cookbooks. He then scoured the literature looking for studies showing an association (positive or negative) with cancer and found that 80% of the ingredients had such studies, often with studies linking them to cancer and others showing a protective effect. As I said at the time, that’s why it’s important to aggregate data. Whenever it comes to studies of diet and virtually any health outcome, there is always a lot of noise.
There is a lot of noise in Kohler’s study, too, but the results are consistent. You can reduce your risk of cancer by staying active and exercising, eating a healthy diet with a lot of plant-based foods and minimizing intake of processed meats, limiting alcohol consumption (although I think the WCRF/AICR guidelines go a bit too far in saying that you shouldn’t drink at all if possible), and maintaining a healthy weight. (Of course, if you stay active and eat a healthy diet, maintaining a healthy weight will probably not be a problem.) Conceptually, it’s easy to do. In practice, as I’m discovering, it’s anything but easy.
No, no, no Orac--it’s the “toxins” that cause cancer, don’t ya know? The toxins in the food, to be more precise. All those kemikillz and stuff. So said my neighbors at a recent party (a couple of whom have cancer) where I was shouted down for suggesting otherwise. All of them drink excessively, many smoke, and the menu was brats, gooey macaroni-type “salads”, lots of white bread, and plenty of sugary treats--and don’t forget the Nachos! Not one walks any further than the driveway.
I’d pass this on, but they wouldn’t get past the first paragraph. On a brighter note, good for you for your efforts. Stay with it and you will develop a palate that starts to prefer the new menu. Enjoy things you like, just watch the portions : )
brats? They were eating unruly children?
It's difficult to lay off the folic acid since it's added to everything.
You should encourage such neighbors to be especially vigilant about their intake of dihydrogen monoxide. In addition to being potentially fatal if inhaled, DHMO is a constituent of many toxic substances and is found in all cancer cells.
When integrative medicine or CAM alone offers nutrient options that have pronounced beneficial physical effects, I wouldn't call that "co-opted".
Targeted nutrition systems are often multi-step affairs for individuals to produce measured, desirable effects and outcomes. In cancer, it currently requires a lot of longitudinal data, way beyond NCCN guidelines to actually steer.
Whereas, mainstream medicine, like NIH, can't even do simple, basic single step work. After 70-80 years, mainstream medicine can't even get it together to do a meaningful kill test on *any* simple acute virus with IV vitamin C, say ~1 gram/kg 3x in a day for 1.5 - 3 days until cleared.
@prn,
Please cite a DBPC study showing a significant reduction in the duration of the common cold from high dose vitamin County.
How much does going from 0.5 g/kg to 1.0 g/kg improve the results.
It's called the dose-response effect.
And isn't "integrative medicine.... alone" an oxymoron?
Andrew Dodds, can you think of a better way to manage them? It would certainly put them on notice.
@ORD,AD: It would fit in well at the church whose bulletin allegedly promised a church meal consisting of a "traditional New England boiled sinner". And you thought Baptists were strict....
@Eric Lund
That reminds me of an ad I saw offering a dog for sale in the local base newspaper
re Orac's personal regime
after an injury almost 6 months ago and a re-injury ( don't ask!) I find that I can no longer keep my weekly routine
( which involved tennis and a dance class) HOWEVER for some odd reason I find that I did not gain any weight AT ALL!
I also began some additional work involving my literary skills which is sedentary ( so is counselling)
My best guess is that I was eating MUCH more to fuel my physical activities and I just am not that hungry now. I also try to ride a stationary bike at home every day as well as doing physiotherapy exercises.
So good luck Orac!
As someone who has had experience with stressful work situations and longer hours I believe that that alone can lead to higher intake of calories - just like having high level of physical exercise.
I am below 25 BMI but sometimes want to try to lose 10 lbs or so in order to put less stress on my ( healing) injuries.
That and tight trousers which beckon me from magazine pages.
@prn #5:
I expect you have rabies in mind.
Layperson here who has been trying to figure out what advice is sound and what's crazy in the sea of bro science everywhere.
I keep discovering that various recommendations are not valuable in and of themselves, but are used to try and prevent some other harmful behavior. As a result, it makes me suspicious of all recommendations -- unless I know why the action is a benefit in an of itself, I question whether it has any real value.
Exercise builds muscle, strength, flexibility and function. Great -- I'm happy to keep up my daily hikes and 3x/week lifting sessions. When it comes to diet, though, I still can't cut through the fog of advice based in some vague morality (you "should" eat veg rather than cheese) vs. advice that shows why specific foods are uniquely good for you.
So when told I should be eating 2.5 cups of fruits or vegetables a day, is s the benefit:
a) tons of fiber,
b) safe calories that will keep me from eating crap calories and help you not add weight,
c) specific nutrients only available via fruit/veg, or
d) some combination of all the above?
I've got A covered through other means and B is something I handle through lifestyle and discipline, so I don't need a food nanny saving me from myself. And if it's C, well, no one ever seems to explain it very clearly. I want to do the right thing, but I also don't want to find out what I'm doing is based on opinion or coercion rather than fact.
Overall, I have to wonder if the basic ACS advice really boils down to (in order of importance): 1) don't smoke, 2) exercise regularly, 3) maintain a healthy weight. How anyone achieves those goals, however, might not make any difference at all.
Partially, yes. It could also be lack of certain ingredients in refined foods, or the destruction of certain ingredients in cooked foods.
Two compounds synthesized almost exclusively in cooked foods are carcinogenic: polycylic aromatic hydrocarbons, and acrylamide. So if you want cancer, grilled hotdogs are second only to a benzene martini.
PS Nice article ORAC, I was half-expecting you to somehow deny the cancer-diet link. Maybe someday you will be forced to admit that diet can also be therapeutic.
MD Account @12: Based on my maternal child nutrition class (so not 100% applicable to everyone, but pretty good) the answer is D: minimally processed (chopped/cooked/fermented) vegetables and fruits are high in fiber (good for many things including pooping and cholesterol) and relatively low in calories, which is important in our current state of abundance. Most foods have vitamins and minerals that your body can use.
Gilbert #3: given the consequences of inadequate folate or folic acid, it should be in more things.
prn @5: Viruses are not alive, therefore they cannot be killed. Your study is impossible as described and we have told you that several times. You can't *see* a virus 'being killed'; they are too small and the biological and chemical processes don't work that way.
JustaTech #14: This is exactly why I get so frustrated. If the actual answer is that I need X amount of fiber, Y amount of specific nutrients and a healthy weight, then I want to be told that first, and then offered the 2.5 cups of fruit/veg as one way to achieve it. It is not the only way, and people need to know the actual target, not a rough direction to aim.
squirrel elite: Please cite a DBPC study showing a significant reduction in the duration of the common cold from high dose vitamin County.
MSM has the funding and patients in need with some level of severity and longer duration. As I stated, decades overdue. Historical examples include viral pneumonia, flu, and mononucleosis. I'm sure NIH and CDC could locate other viral patients with enough severity and projected average duration. If they really wanted to.
How much does going from 0.5 g/kg to 1.0 g/kg improve the results...It’s called the dose-response effect.
Maybe a lot. I think the approximate threshold of reliability is considered 0.7 g/kg for the historical viruses.
And isn’t “integrative medicine…. alone” an oxymoron?
CAM MDs and NDs don't have to be a member of the mainstream team to integrate unique therapies, although msm cooperation might be in the patient's best interest. This seemed to happen in varying degrees with cancer care 10 years ago. I'm not watching such US politics now.
You can see the corona virus with a light microscope, but the other viruses are deactivated by the electron beam itself [I think] in electron microscpopy. This means that the operator is always picoseconds too late from viewing active viruses.
This is not particularly surprising given how powerful the effect of smoking is on lung cancer risk and how uncommon lung cancer not associated with smoking is.
I've heard that if smoking did not exist, the incidence of lung cancer would only be cut by half. Is that not true, or close to the truth?
JT, re: killed
Sounds like cheap point scoring on pedantics. Killed, in lieu of longer phrasing on qualification or conditions of clinical cure. Even some vaccines are commonly referred to as killed virus vaccines.
While I appreciate your help and more experienced view on the labs, other lab researchers seemed to indicate the measurements were possible.
Q: When did the lung cancer anti-smoking campaign really take off?
A: When the US was doing hundreds of nuclear atmospheric tests.
Q: Who was behind the lung cancer smoking campaign?
A: The US government.
Tobacco has been scapegoated, but it still contributes to lung cancer somewhat. The lords of coal-burning and nuclear testing no doubt try to shift the blame on tobacco to avoid liability.
I am smoking organic tobacco right now and I'm not particularly worried about getting cancer. I quit my chimney-sweeping job years ago.
Eric Lund say (#4),
DHMO is a constituent of many toxic substances and is found in all cancer cells.
MJD says,
DHMO may have benefits, For example, U.S. Patent 9,173,899:
Method of preventing and treating autistic spectrum disorders (Lo, et al. Patent number 9,173,899 – November 3, 2015)
Abstract - This describes a method of treating autistic spectrum disorders that includes administration to a person of a product, which contains stable water clusters, such as stable double helix water clusters, by taking the products by mouth, applying the products on a skin of the person, in taking the product by breathing, introducing the products intravenously.
Claim 11 - The method of treating an autism spectrum disorder as defined in claim 1, further comprising determining on the body of the person spots which are associated with the acupoints and which are hot in that they have a surface temperature that is higher than a surface temperature of an adjoining surface area, and wherein said applying includes applying the product with the stable water clusters on the acupoints associated with the thusly determined hot spots on the body of the person.
The inventor explained that the products with the stable water clusters are applied on the body of a person on acupoints, which lie on meridians of a meridian system of the person. Furthermore, hot spots and hot areas on the body of the person can be carried out with the use of an infrared imaging system that takes thermal images of the person.
David L. Gann (second inventor listed with a co-inventor) founded D&Y Laboratories Incorporated. Mr. Gann received a Bachelor’s degree in science with post-graduate work in physics. Mr. Gann has organized educational symposiums on crucial environmental issues, including global climate change and nuclear waste cleanup in conjunction with the United States Department of Energy and Los Alamos National Laboratories.
D&Y Laboratories Incorporated (current assignee) has protection for United States patent 9,173,899 (Lo, et al.) to November 25, 2033.
Ohh yes, JustaTech; The dreaded neural tube defects, spina bifida, and anencephaly is still a narrow justification. And besides, doctors no longer prescribe 'folic acid' for pregnant women but instead give real folate (5-methyltetrahydrofolate/levomefolic acid)
It is a distasteful practice to be mandating introduction of it into every flour and cerel grain since 1998, often when it is not required to do so. I guess, it is a marketing ploy for the consumer to see large amounts of folic acid on a product — The reality is that it is probably an addative to be avoided, like too much sodium for some people.
The1943 petroleum-derived *folic acid* must first be metabolized through dihydrofolate reductase (this is done in the liver and is a pretty low rate of conversion). It is also much more bioavailable crosses through the intestines much more readily than natural folates --. Unmetabolized folic acid downregulates absorption and processing of the active form, levomefolic acid, as it builds up in the body. Many in the populace are not able to convert folic acid because of being old or lacking the necessary genetics to do so.
http://scholar.google.com/scholar?q=unmetabolized+folic+acid&hl=en&as_s…
In the past, I’ve pointed out that it may be veiwed as selectively absorbing Cheetos as a child. Then the child is not hungry at dinner. I also equate this mandated ubiquitousness of the chemical to be Vonnegut’s Harrison Bergeron; Only it is the Life Expectancy and Quality General instead of the Handicapper General — That those with poor nutrition generally expect a higher quality of life and longevity with the supplement but those with good nutrition have those values derated.
With widespread consumption of processed foods and ubiquitous inclusion into just about everything* else, I’m convinced we’re getting too much with all that entails.
*I note that a particular house brand of instant oatmeal contains a whopping 20% Folate (as folic acid); The house organic brand lists 2% folic acid but does not show it included in the ingredients as this is the real folate — There is serious conflation and confusion on the two terms.
@prn 15,
That would be fine except that Vitamin C has been studied many times for treating or preventing the common cold and the results are minimal at best.
http://www.webmd.com/cold-and-flu/cold-guide/vitamin-c-for-common-cold
So if you assert a benefit greater than reducing the duration by a day or so, please provide the evidence to support it.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3218540/
Interesting. There are many ways that synthetic folic acids differ from the folates found in vegetables and fruits. All of the natural folates exist in one steroisometric form: (S)folate, which rotates a plane of polarized light counterclockwise. Synthetic folic acid exists as a racemic mixture, and only Merck has synthesized an all levorotary product.
Synthetic folic acid is fully oxidized, while the natural forms are at least twice reduced.
Folates in vegetables and fruits have a methylated nitrogen on the pteridine ring and synthetic folic acid does not.
No doubt these differences arise out of necessity and cost. Folates are one of the most complex and difficult to synthesize vitamins.
Hey Squirrel,
You realize that those reports are totally irrelavent to what I said, don't you?
Oral doses from 200 mg to perhaps 1 gram 1-2-3 times a day, where most of their data were even lower and slower, vs 1 gram/kg dosing several times a day... Much different results.
Mostly this discussion is to inform you what the issues are. Maimstream medicine gets the C discussion so wrong, it hurts many people several ways. Basically most infectious disease reports of injected or IV megavitamin C are about cases and series. There are only a few trials at too low doses to be a reliable treatment, e.g. 1 gram injections.
A good stiff dose of IV vitamin rapidly knocks down the effects of acute viruses. Several more or perhaps a drip probably handle most people in the first 36-72 hrs or less of some fairly nasty things like flaviviruses.
I do think MSM should do the trials for the unwashed masses. At this point we mostly don't need MSM help, other than to stay out of the way.
@prn: So the plan for the common cold is to take vitamin C in industrial doses until you're sick? I bet if you're hospitalised for this IV "treatment" and then puking your guts out because you reached toxicity, you're not thinking about your cold anymore!
@Szilard: That's funny, because the USA is not the only country in the world where scientists worked on the smoking/lung cancer link... But hey, why avoid a bit of conspiracy theory?
BTW, I bet the "coincidence" between atomic tests and identification of a link between smoking and lung cancer is down to the effect of mass production and consumption of cigarettes since around the beginning of the 20th century. The incidence of cancer just took time to build and become preoccupying. As it often is with cancer.
@20
Says he conveniently ignoring the role that British epidemiologists played in identifying the links between smoking and lung cancer...
Need to get a better conspiracy there...
Oh, and what difference does "organic" tobacco make? Less nicotine? Fewer particulates? What?
Irene,
Puking due to the IV vitamin C is not common. If one does puke, other problems are likely more contributory.
Oral vitamin C is an excellent laxative if you finally exceed bowel tolerance. Bowel tolerance does elevate with the severity of an illness and was so described in a paper by Dr Robert Cathcart. For example, a 100 lb person with severe mononucleosis may tolerate 150-200 grams of oral vitamin C on the first day taken vs 10-20 grams in good normal health)
Also sick people who are severely vitamin D deficient will more or less stay sickly, even if they tamp down their viral infection. Vitaimin C doesn't solve all problems.
Organic tobacco has no pesticides, and less heavy metals. Tobacco likes to accumulate cadmium and radium found in phosphate rock fertilizers and this isn't used in organic farming.
http://www.ncbi.nlm.nih.gov/pubmed/285289
You cannot deny that nuclear fallout causes lung cancer. This theory is not as crazy as it sounds.
If nuclear fallout causes lung cancer, instead of smoking, why is it that mainly smokers get lung cancer?
And the fact remains that one can do everything right and still get cancer, despite having no family history, and being too young by a couple of decades. All the vitamins, exercise, fruit, vegetables, whole grains, and green tea in the world cannot necessarily prevent that. And they certainly cannot cure it. Surgery and chemo do. Diet and exercis did make those things easier to bear, but they do not cure cancer. Medicine does.
@Szilard- I have some low-calorie drain cleaner if you're interested.
# 28 Murmur
Says Murmur
/Says he conveniently ignoring the role that British epidemiologists played in identifying the links between smoking and lung cancer… conveniently ignoring the fact that the UK was in on the conspiracy due to its nuclear tests.
Ignore that fact that the tests were in Australia.
Redblues,
What I've seen in the current state of the nutritional art, is to get immunological responses that made surgery more effective and to make normally futile surgery, productive. I seen terminal patients that look better than their "healthy" contemporaries, and not get sick when the latest plague sweeps through town or the house.
I've seen chemo made radically more tolerable by nutrition, from early failure due to toxicity to higher dosage, and made less chemo perform better than the usual chemo, for far, far longer. This is not new and the Japanese have long had a simple version that they call immunochemo.
As for prevention, I think current ADA-style nutrtition is a long, long way from realizing the potential of nutrition. Certainly popular nutrition (mal)practices, including diabetic obesity forming amounts of carbs, no matter how clucked over, can radically accelerate cancer development and processes. Never mind the fundamentals, enzyme inhibitors and immune modulating effects available in nutrition.
Not only doctors are aware of the effects of diet and exercise (contrary to the alt-med narrative) but confronted to obese patients, according to a recent survey, they tend to focus on weight without due consideration of other factors.
http://mobile.nytimes.com/2016/09/26/health/obese-patients-health-care…
Mary Darling @15: The challenge is that nutritional science does not know what you Mary need as far as X grams of fiber. It might be X today and X+0.1 tomorrow, based on a change in your diet, activity, infection, air quality, who knows. Nutrition is incredibly hard to study because you are working with a hugely diverse population, whose needs change dramatically over time.
So the best that can be done for almost everyone is a set of general recommendations that are (hopefully) easy to follow.
For people with very specific disorders it might be possible to make that very specific diet you asked for, but it requires a huge amount of resources (tests, computers, experts), so unless you are dying from your diet, generally it's not done.
Yes, but there is always a cause no matter how cryptic. Newtons 1st law of pathophysiology states:
It is much easier to give rats lung cancer with plutonium than with tobacco smoke:
Rats ≠ humans.
It's always been known to be more difficult to induce lung cancer with tobacco rodents. However, the epidemiological evidence that smoking causes cancer in humans is so overwhelming as to be bulletproof.
Szilard @39: Are rats an appropriate animal model of human lungs? I though researchers usually used pigs or ferrets for human lung diseases?
I am sure that you are familiar with all of the other negative health outcomes of breathing any kind of smoke (tobacco, weed, wood, coal)? The kind of thing that substantially shortens the lives of women all over the developing world who cook over smoky fires?
Gilbert @22: Yes, and folic acid has just recently been added to foods made from corn masa (tortillas mostly) to reduce the rate of neural tube defects in American communities that eat more corn masa than wheat flour or rice.
I'm sorry to say that I am not surprised that you don't think that devastating or fatal birth defects are a bid deal.
JustaTech, I smell ol' toe jam for brains.
@prn,
There are lots of studies, enough to merit 3 Cocharne reviews.
https://www.ncbi.nlm.nih.gov/pubmed/23440782
The results show a modest preventive benefit, but no therapeutic effect.
I'm willing to be persuaded but you have to show me the evidence.
Doug, Yeah, probably, but I was just reading about how many years of life are lost to respiratory illness and damage from cook-stove smoke and it bugged me.
I really want to snark about the tobacco thing, but I can't find a way to do it without sounding like a total jerk about addiction.
The facts are clear, radioactive α-particles are way more carcinogenic that tobacco smoke, but the tobacco-cancer link gets way more publicity.
The US government was responsible for hundreds of atmospheric nuclear tests and would have a motive for emphasizing the tobacco-cancer link and de-emphasizing the radioactive fallout-cancer link.
Is this a website where every hint of conspiracy is ridiculed, except when "quacks" do it? Is the mission statement of this blog to absolve the government and medicine of any wrongdoing whatsoever?
I could list numerous examples of government lies and medical mistakes. These things are in no way out of the ordinary. I get the feeling that everyone here is reading out of the same handbook that tabulates which positions to endorse and which positions to ridicule.
"Newtons 1st law of pathophysiology states:
In an inertial reference frame, a person free of cancer will remain so unless acted upon by a carcinogen."
Errors during DNA replication may also result in changes leading to cancer - the replication process isn't perfect, even in the absence of a carcinogen.
To JustaTech, re: #37:
Thank you for taking the time to reply! I do understand the challenge of personal specificity (how much of X for an individual) but the same holds true for anything -- including setting a recommended amount of fruit and veg, that might be right for a 150 pound male but all wrong for a 250 pound diabetic.
My complaint is that guidelines all too often list the how (2.5 cups of fruit and veg) rather than the what (adequate fiber, specific nutrients and healthy weight). As someone trying to build an optimal exercise and eating program, what I first want to know is what I need. Some further thoughts on how I can achieve it are helpful, but not the same, especially when they never clarify the real goal.
On the exercise side of things, the NIH says I need a 150 minutes of exercise that generates a heart rate of 50% to 70% of MHR. This is far, far more helpful to me than if they'd simply said, "walk 1.5 miles a day." It's specific, it provides the actual result that helps (elevated heart rate) and it gives me the chance to figure out the best way for me to achieve it. Telling me to go for a walk, on the other hand, may not get me what I actually need (if my heart rate stays low) and may keep me from trying other avenues to reach the real goal.
Nutrition is already an inexact science. It's credibility -- and influence -- is further compromised when advice is overly specific without providing the detailed context on which it's based.
@Szilard,
Noone denies that alpha particle radiation is a lung cancer risk.
But unless you'really a miner, do a lot of spelunking, deliberate go seeking radon exposure for its "health" benefits, or spend a lot of time in a poorly ventilated basement, the average person's alpha dose is low.
I made alpha emitter samples 35 years ago and I still haven'T gotten lung cancer from it.
But, more importantly, the big drop in lung cancer in the last 30 years wasn't because more people were living in houses without basements.
Ohh, think of all the saved baby spines, JustaTech #41. Still, the FDA had to be lobbied to 'allow' the addition as it was first suspected that the chemical would not be stable through the heating that corn masa products go through.
http://www.npr.org/sections/thesalt/2016/04/15/474388880/coming-soon-to…
Basically the move is a marketing ploy, as I said in #22. It may prove interesting setting a start date to track the rates of autism in Hispanic communities now -- 1998 gave us several things; It gave us removal of thimerisol, introduction of GMO and Roundup saturation, and overfortification with folic acid. I wonder if two of these things have hidden a decline from the first.
Raw folic acid in the circulatory system builds up and interfers with normal folate uptake and metabolism. Futhermore, it is difficult to clear thus making it a kind of chronic poison.
Re Szilard and Newton's First Law of Pathophysiology - You omitted the critical note. The full text reads:
"In an inertial reference frame, a person free of cancer will remain so unless acted upon by a carcinogen.
Note: All organisms are exposed to carcinogens."
I could list numerous examples of government lies and medical mistakes
And will no doubt do so, under a variety of nyms.
Szilard -- radon gas exposure has long been one of the major causes of lung cancer. I fail to see why that should forestall efforts to eliminate the other one, especially since reducing tobacco usage is much easier than radon remediation.
Gilbert, #50
United States wasn't the only country to remove thimerasol from vaccines. Sweden and Denmark did it in 1992-1993 and England (UK?) did it around 2004. Different countries and widely different times.
Did those countries expierence a drop in autism? Did other countries who dropped thimerasol expierience a drop in autism rates?
jrk @34
Those damn sneaky alpha emitters from the UK-ian atomic bomb tests at Maralinga were cunning enough that they managed to make their way ONLY to the UK from Austrililalia...And once here fool the likes of Richard Doll by impersonating the effects of tobacco smoke (non-organic of course...)...
Seriously though, many UK citizens are well aware of the deleterious effects those nuclear tests had on our military personnel who were present and the long fight for recognition of that and compensation. That and the piss poor cleaning up of the site.
None of which has any relevance to the prevalence of lung cancer in the UK itself...As pointed out radon is more of a problem in chunks of this country (why, yes, that it a huge piece of granite I can see off in the distance from my front window...) than anything from nuclear testing (hint - how far do most alpha emitters actually travel in the air?)
From what I gather, the only way to avoid being exposed to carcinogens would be to seal oneself in a sealed, airtight, lead-lined container. (That would certainly guarantee that one would not die of cancer.)
Grey Falcon #56
Yes, you wouldn't die of cancer, you'd die much more quickly of asphyxiation or starvation.
But seriously, you obviously haven't pondered alison #47 : it seems that a large number of cancers cannot be associated with any environmental or dietary factor, and just occur, effectively spontaneously. In other words, just bad luck. This is something modern homo sapiens is often in denial about.
Mr. Dugdale, why did you feel the need to explain my joke to me?
@Grey Falcon,
Perhaps it was a bit subtle.
It does remind me of the claim made a while back that the normal level of radiation had a protective effect. But the only way to really demonstrate that would be to raise animals in an ultra-low radiation environment like a salt mine and compare. And even if it did, we're not going to move the world's population into underground radiation shelters anyway.
The radon mines out west are supposed to work by elevating ones' radiation temporarily thereby doing *something* to the immune system. http://www.radonmine.com/why.php
There is one thing about radon that should be noted -- Since it is a gas, it is a transient exposure and does not 'embed' in tissue and continue to irradiate.
================================
http://joe.endocrinology-journals.org/content/224/3/245
Grey Falcon -
sorry, my irony meter is in for repair.
That was marginally plausible back in the 20's.
We can't pretend any more.
With a half life of 3.6 days, there's a good chance it will decay while it's in you, and then you get to worry about the Polonium, Bismuth and Lead.
Can you say radioactive heavy metals?
http://www.ccnr.org/radon_chart.html
Polonium, Bismuth, and Lead.
Ouch! I knew it was the densest gas but I did not know that.
As an anecdotal, I was 'cured' in a cave. I had bad bronchitis and the doctor tried steering me away from a 3-day scouts trip by telling me I would not survive. Damp, dusty, cured, I was. I don't recall if there was an antibiotic but I don't remember taking it. In fact, there have been a few times when chest congestion was cleared after a few hours in a cave -- Perhaps, it could be due to the absence of ozone?
Sine you like videos, think
"every breath you take, I'll be decaying in you"
https://youtu.be/OMOGaugKpzs
There are lots of studies, enough to merit 3 Cocharne reviews.
The results show a modest preventive benefit, but no therapeutic effect.
Those are the extremely low dose studies, I mentioned.
I am not here to p=0.01 "prove" to you per se on the basis of preliminary individual reports. Merely I wish to inform reasonable people of the massive difference of inputs to yield the claimed results that bear closer inspection. The nature of the beast is such that astute individuals can benefit ahead of the information lag or drag pretty dramatically and have for decades on this specific issue.
Mary Darling @48: I'm really not an expert so I can't offer any better explanation.
If you're interested in learning more there have been some great nutrition classes on Coursera (and maybe also EdX) that you could take.
Reading your blog makes me very sad. My 9 years old son was given a death sentence in march 2015. He is still alive today. Ive been giving in to most alternative treatments you spend your time shitting on. I may not save him, but i have hope and we are fighting. You vomit pus.
And then one day, you will be giving your own death sentence. Let's see what quakeries you indulge in, when doctors give you no hope.
Thanks for not fully taking the bait from the organic-tobacco-product-using poster above. That restraint repeatedly adds to the value of this blog.