
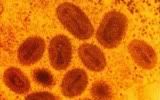
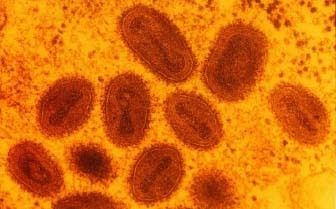
 Smallpox is, without a doubt, the biggest success story in all of vaccination. The practice of variolation, or the purposeful inoculation of naïve individuals with material from scabs of smallpox victims, was practiced for years prior to Edward Jenner's substitution of cowpox for the smallpox (Variola) virus. The vaccinia virus, thought to be a derivative of cowpox, has been used in the 20th century in smallpox vaccination campaigns. Vaccina elicits antibodies that protect from smallpox infection, yet typically causes an asymptomatic or only mildly symptomatic infection. This worldwide effort led to the last known naturally-occurring case of smallpox, which occurred in 1977 in Somalia. (The last known U.S. case dates back to 1949). However, in the aftermath of 9/11 and fears over the use of bioweapons, the U.S. military instituted the controversial smallpox vaccination program, as part of the Department of Defense's "national strategy to safeguard Americans against smallpox attack." To date, over a million service people have been vaccinated. This program has been in the news several times recently, as vaccinia infections have spread beyond the vaccinated individual and to family members and now, sexual partners. More after the jump.
Smallpox is, without a doubt, the biggest success story in all of vaccination. The practice of variolation, or the purposeful inoculation of naïve individuals with material from scabs of smallpox victims, was practiced for years prior to Edward Jenner's substitution of cowpox for the smallpox (Variola) virus. The vaccinia virus, thought to be a derivative of cowpox, has been used in the 20th century in smallpox vaccination campaigns. Vaccina elicits antibodies that protect from smallpox infection, yet typically causes an asymptomatic or only mildly symptomatic infection. This worldwide effort led to the last known naturally-occurring case of smallpox, which occurred in 1977 in Somalia. (The last known U.S. case dates back to 1949). However, in the aftermath of 9/11 and fears over the use of bioweapons, the U.S. military instituted the controversial smallpox vaccination program, as part of the Department of Defense's "national strategy to safeguard Americans against smallpox attack." To date, over a million service people have been vaccinated. This program has been in the news several times recently, as vaccinia infections have spread beyond the vaccinated individual and to family members and now, sexual partners. More after the jump.
This past March, reports surfaced regarding a 2-year-old Indiana boy. His father was in the Army, and had recently received his smallpox vaccination. The vaccinia virus contained in the vaccine is a live virus; therefore, it is capable of replication in the recipient, and potentially of spread to others. This is exactly what happened in this case. The father sread it to his son, who developed a rare side effect: eczema vaccinatum, essentially a crusty skin rash caused by the virus in those who already suffer from eczema. In the boy's case, the rash eventually spread over 80% of his body, and the condition can be life-threatening. (Indeed, the boy was on a ventilator for a time, and doctors predict he'll lose up to 20% of his outer skin layer). The boy's mother also contracted the virus, although a much milder case than her son.
Now, just this week comes a report of sexual transmission of vaccina virus. An Alaskan woman and another U.S. soldier engaged in "manual stimulation and vaginal intercourse" three days after the soldier had received his smallpox vaccination. A month later, the woman reported to her doctor with vaginal sores. As her symptoms worsened and were unresponsive to treatment, doctors took swabs from the lesions and submitted them to both the state health department and the CDC, who determined the virus present in the swabbed material was a match to vaccinia.
While these are only two cases out of over a million vaccinated, they are instructive in that both could probably have been prevented. Eczema is one risk factor for development of severe illness after vaccinia infection; therefore, vaccine recipients themselves are questioned about history of eczema, and are reportedly cautioned about avoiding others who are known to have a similar history post-vaccination. The newspaper article says that the child was known to have such a history; therefore, his father should have been cautioned to stay away from him in the days following vaccination. Whether he wasn't told, or simply didn't understand and/or pay attention isn't known, as far as I could tell.
With the second case report, contact vaccinia is much more common than the serious eczema vaccinatum that the boy developed. However, this also could have been prevented with more information. The Morbidity and Mortality Weekly Report (MMWR) write-up states:
Since March 8, 2007, CDC and the U.S. Department of Defense have received reports of four instances of nongenital contact vaccinia associated with recently vaccinated service members, including two cases from Indiana and one case each from Alabama and New Mexico.
and the CIDRAP article states:
According to the US Department of Defense (DoD) Web site, 61 cases (36 lab-confirmed) of contact vaccinia occurred, mainly to spouses and adult intimate contacts, between Dec 13, 2002, and Apr 12, 2007.
This suggests that more education, with a stress on avoidance of close contact in the post-vaccination period, could have prevented these cases.
In the broad scope of things, these really are only a handful of cases, particularly given the large number of servicemen and women who've been vaccinated to date. However, as vaccinia requires close contact to efficiently spread, an emphasis on these cases and the need to keep a bit to one's self in the post-vaccination period is something that simply doesn't hurt to emphasize. It also has served to cause those exposed to question the need for a vaccination program in our military, since smallpox is one of the few pathogens where post-exposure vaccination can still stop the onset of disease.
Image from http://www.humanillnesses.com/original/images/hdc_0001_0003_0_img0246.j…
{kind=link}
Dear DT,
How do you envision the cell biology behind the idea and your statement above that "HIV" causes anemia? Do the little "HIV" virons insert their RNA into the red blood cell nuclei? Same question for wasting and muscle cells, neurons, heart disease in the pre-HAART era, liver disease (which above I posted as what Bica et all claim is the leading cause of death in their "HIV" population which none of you want to even discuss)?
Dear Franklin,
Thanks for the complement above. So this blog exercise has been useful to you also after all. I believe blogs like Tara's here are places to "air out" different sides of an argument-especially arguments as heated as ours regarding "HIV" and "AIDS," before putting anything into the peer-reviewed literature.
Also, thanks for reading "The ABC's of AIDS denialism" piece. It was an attempt of mine to simply point out that every so-called AIDS expert or organization that promotes the "HIV/AIDS" paradigm has at some point violated the simple logic that A (HIV) leads to B (immune suppression) which leads to C (AIDS-defining illness and death). These folks, however, are not called Holocaust deniers, dissidents, denialists, liars, criminals that need incarceration and censorship (as Wainberg suggested recently), etc. Instead, inconsistencies or violations in the simple A leads to B leads to C paradigm were not discussed and were ignored, nor were any steps made to reconcile them through futher experiments, open debate, or policy decision changes. The ABC logic I used is no different than what I use to discuss cancer, or any other scientific or medical hypothesis.
E.G. Cancer cells cause cancer. Not in growing embryonic fields they don't. Some patients have spontaneous remissions for reasons we do not understand but need to understand because nature may be giving us a hint as to how to more frequently reverse the syndrome(s).
A( cancer cells) lead to B (tumors), which then kill everybody.
Wrong. A (highly invasive and metastatic melanoma cells) placed into the developing neural creast of an embryo) lead to the formation of normal dorsal root ganglia and other tissues).
Cancer denialism at its best. Don't you agree. Incarceration? Holocaust denial. Cancer dissident. Censorship?
By contrast, I noticed that in the Bergman and Moore film that just was posted about the mission of AIDSTruth to root out us "HIV/AIDS" Holocaust-denying terrorists from spreading lies and misinformation, that Bergman said something to the effect that (with all of her scientific training); "It may have been a mistake to hit early and hard," while Moore mumbled something about "well ARVS are like cancer chemo, and it isn't good to sprinkle them on your cornflakes" (these aren't exact quotes so don't have a seizure if I got a word or two wrong-but the word(s) "was wrong" and cornflakes" were definitely mentioned. I can't stand to watch it again to get the exact words-because there is no apology, no concession on their parts, to the thousands who were and continue to be lied to about the "life-saving" nature of ARV's. Talk about lies and distortions!
Regarding accuracy of quotes-I've tried to make concessions on this blog to you and your gang in order to look differently at or correct important conclusions extracted from a blizzard of highly censored "HIV/AIDS" work, to see if my conclusions need any adjustments or revisions, and to see if any progress is possible through give and take-because this stuff should be presented in its most simple and direct form.
For instance, some time ago, I got it wrong when I said that Hepatitis B was used as a surrogate marker for "HIV" infection early during the AIDS era. This statement was derived from the fact that I read:
"Hepatitis B virus is found in 90% of drug addicts positive for antibody to AIDS virus" (Peutherer et al., HTLV-III antibody in Edinburgh drug addicts.
The Lancet 2: 1129-1130, 1985).
After seeing this in a blog, Martin Deleney wrote to me and corrected me regarding this "misinformation" when I said on another blog: "Hepatitis B was used as a surrogate marker for HIV infection early in the AIDS era."
What I said is incorrect, and what Deleney said is correct, and I thanked him for the correction. I changed this in my ABC's piece you mentioned before it was posted anywhere.
"4g. Baruch Blumberg, D. Carlton Gadjucek, and development of molecular (recombinant vaccines):
Currently, "hepatitis B," (and "hepatitis C" but less efficiently) is supposedly transmitted like "HIV." Also, like "HIV's" touted ability to cause 6 cancers, "hepatitis B" is thought capable of causing a type of liver cancer known as hepatocellular carcinoma, according to the CDC, the WHO, and other Public health agencies. It is also supposed to affect the same "risk groups" as "HIV." It was also first thought to be the best surrogate marker of "HIV" infection (Martin Deleney, Project Inform, Personal communication) in some of the first cohorts of U.S. and Scottish AIDS patients:
"Hepatitis B virus is found in 90% of drug addicts positive for antibody to AIDS virus" (64).
If you guys want to get hot and bothered over exact quotes about a blizzard of papers based on distortions, and pharma-backed interests, try revising the following quotes (litanies) for their truth content, that are taught to our junior high school children, promoted and trumpeted by public health services, the WHO, the CDC, etc.
"It is timely and cost effective to now test every man woman and child for HIV."
"HIV is like getting hit by a truck-you need no co-factors."
"AZT is a life-saving ARV."
"Everyone is equally at risk of acquiring HIV."
"There are good animal models of AIDS."
"The average life-expectancy of AIDS patients has increased to 24 years, if you pay 350,000 dollars."
"As much as 40% of some populations in Africa are infected with HIV, the virus that causes AIDS."
"HIV causes Kaposi's sarcoma."
"HIV can be isolated from everyone who has AIDS."
"HIV causes cervical cancer."
"Smoking increases the risk of acquiring HIV, British researchers found."
"Long-term drug addition has nothing to do with immunotoxicity or the acquisition of AIDS-defining illnesses."
"8,000 people die of HIV acquired AIDS every day."
"Circumcision reduces acquisition of HIV by 47%."
"Nevirapine reduces risk of HIV acquision in MTCT."
"David Acer infected 3 of his several thousand dental patients with HIV."
"Rudolf Nuriev died from AIDS."
"Eliza Jane Scovill died of AIDS"
"Arthur Ashe died of AIDS."
"YOU and your child are going to die of AIDS unless you subject yourself and your infant to ARV's."
Instead of playing point-counterpoint, let me simply ask you directly what you think the following means-it will save time:
The DAIDS 1997 official "HIV" culturing manual, under quality control, Section VI, page 45, advocates, "Do not use PHA stimulated PBMC older than 3 days post stimulation" when testing them for the absence of "HIV" from your healthy donor source.
Why not? Isn't it important to treat control cultures exactly the same in both duration and in what is added (PHA,etc.) in order to come to any conclusion about the experimentals?
Why did Gluschankof et al., say the following?
Gluschankof P, Mondor I, Gelderblom HR, Sattentau. Cell membrane vesicles are a major contaminant of gradient-enriched human immunodeficiency virus type-1 membrane preparations. Virology 230: 125-133, 1997).
Did Montagnier and his colleagues imply in their 1991 Virology paper:
Mitogenic stimulation and activation, in control cultures in the absence of HIV, can induce the same cytopathic effects as sera or cells derived from "AIDS" patients?
What does this mean?
Did investigators involved in the AIDS Vaccine Program, SAIC, National Cancer Institute-Frederick Cancer Research and Development Center, Maryland, published reports stating that PHA (phytohemmaglutinin) and IL2 (interleukin-2) stimulated healthy cells produce "viral like particles" and HIV 'specific' proteins only when stimulated with PHA and IL-2? Did they also claim that microvesicles were a source of contaminating cellular proteins found in purified HIV-1 preparations, as their title suggests (Bess JW Jr, Gorelick RJ, Bosche WJ, Henderson LE, Arthur LO. Microvesicles are a source of contaminating cellular proteins found in purified HIV-1 preparations. Virology, Mar 31; 230(1):134-44, 1997).
I just want to get these correct before they go into peer reviewed publications. I trust you can help me out here with precision and with interpretation (the way you see it).
Cheers,
Andy
Maniotis says there's a paper by Bess et al "stating"
stimulated healthy cells produce "viral like particles" and HIV 'specific' proteins
Anyone who reads the paper knows, the paper doesn't "state" this. It doesn't say it anywhere or even imply it. Look at table one. Which cells contain capsid an HIV 'specific' protein? Surprise only the ones with HIV. Not the uninfected cells. Actually not any uninfected cells.
Look at figure 1. Which lanes have abundant HIV proteins like capsid matrix and nucleocapsid? Surprise only the ones with HIV.
The authors never find HIV proteins in uninfected cells stimulated or not stimulated.
I posted a review of EMs. Other people added more references. The Bess paper also shows virions are not mistaken for microvesicles by morphology. I said before, immunoelectron microscopy lets you know for sure. Today microvesicles can be separated from virus preps and alot of labs do this. Microvesicles are not virions virions are not microvesicles.
They have things in common. They both have a membrane from the cell. They both have some cytoplasmic stuff inside. Including host proteins.
But alot not in common. The membrane of virions has different distribution of components. The virion selectively incorporates some host proteins and excludes some too.
Maniotis ignores all this to keep up his deception of people who don't know the literature well enough to see him for what he is.
Adle said; Look at figure 1. Which lanes have abundant HIV proteins like capsid matrix and nucleocapsid? Surprise only the ones with HIV.
Are you going to continue to evade, ignore and stonewall the lack of cell damage or cell death involving host cells on the EM HIV studies? Yes we see the cones and lateral bodies and surface knobs, but where is the host cell injury from this awful bug? Surely it must be visible on some of the pics?
For the lurkers, this is tyical behavior for the AIDs toxic Drugs pushers and AIDS political activists.
That's progress patriot. We can conclude from this Bess et al microvesicle paper by itself, HIV proteins are specifically found in HIV virions. HIV infects cells and they can make new HIV virions. Uninfected cells in culture don't make HIV no matter how they're treated. HIV virions aren't mistaken for microvesicles by anyone anymore except a scientist at the University of Chicago, Illinois named Andrew Maniotis.
The questions about damage were answered by other people. Our "patriot" can pretend they weren't or not look at the papers they gave. I guess the goal is, get the "drug company reps" to say slightly different things you can twist and then say falsely we're all lying to you.
Why don't you ask someone to put an electron microscope in a patient's bloodstream and take live pics of HIV killing cells. Maybe a movie??!! Tell em until they do that you're not going to believe it's real! Oh, by the way there are some things just not techincally possible. Just ask the guys at "judicial watch".
Instead of playing point-counterpoint, let me simply ask you directly what you think the following means-it will save time:
The DAIDS 1997 official "HIV" culturing manual, under quality control, Section VI, page 45, advocates, "Do not use PHA stimulated PBMC older than 3 days post stimulation" when testing them for the absence of "HIV" from your healthy donor source.
Why not? Isn't it important to treat control cultures exactly the same in both duration and in what is added (PHA,etc.) in order to come to any conclusion about the experimentals?
On the remote chance that you are genuinely confused and not just being disingenuous, let me spell it out for you.
Control cultures are treated exactly the same in both duration and in what is added.
In order to expand a population of HIV in culture, you need to supply the culture with fresh potentially infectable T cells at regular intervals. (In vivo those fresh potentially infectable T cells are entering the peripheral blood from the lymph nodes etc. ) In vitro they are supplied as PBMC from an non infected source that have been PHA stimulated for no more than 3 days.
So control cultures or HIV infected cultures are 'fed' every 3-4 days with some PHA stimulated PBMC from a non infected source.
Andrew, I never said that, you are confusing me with someone else. Anyway, you know perfectly well (or at least I hope you do, but based on some of your previous claims I wouldn't be too confident about it) that RBCs do NOT have nuclei.
You want to discuss why liver disease is a leading cause of death in patients today? We have been over this data time after time after time. Where were you?
Liver deaths have only become RELATIVELY more common because the mortality from AIDS has plummeted with the introduction of HAART. Most deaths from liver disease (80% in the DAD study) are due to chronic hepatitis C and B anyway, and not from the drugs (although they make a minor contribution).
Hypothetical example to show the math principle in action:
Pre HAART: 3 deaths/100 person years from AIDS, 0.5 deaths from liver disease. (=14% deaths are from liver disease)
Post HAART: 1 death/100 person years from AIDS, 0.7deaths from liver disease.(=41% deaths from liver disease)
Denialist response: Shock! Horror! Evil drugs! Liver deaths have more than doubled!
What a lame attempt to label any scientist who enters discussion about any aspect of HIV science as a "denialist". Rather than your silly analogies, let me give you an example of what you really are implying:
Historian A challenges the breakdown of deaths in Belsen in 1943. Did as many as 30 thousand die from typhus, or were most deaths from malnutrition?
Maniotis response: "Holocaust denier!"
When HIV scientists debate finer points about AIDS pathogenesis, or pharmakokinetics of protease inhibitors, they are not denying that HIV exists or causes AIDS, merely refining hypotheses using the appropriate scientific method.
Andrew, you still seem to be struggling with the concept of quotes. If Dr Jones says "A causes B", then that is what he said, and the statement that Dr Jones said "A causes B" is factually correct even if A does not cause B.
If you feel that Dr Jones should have said something different, you cannot put words into his mouth and say: Dr Jones says "A never causes B or C but can cause D". This is the type of dishonesty your own attempts to cite the literature are filled with.
One or two of these quotes are factually incorrect eg: "HIV causes Kaposi sarcoma". Was this an accurate quote? - Who said this and when? (it may be a quote from the early days of AIDS, when HHV8 was unknown). Science is dynamic, afterall. Who said "HIV causes cervical carcinoma" - Can we see a reference please? I doubt any HIV scientist would say this. I hope you are not being deliberately obtuse here and playing funny buggers with the AIDS definition. [Perhaps you are being honest, and perhaps the person who said it did so in good faith - if so perhaps you could tell us how accurate on a scale from 1 to 10 would you rate this claim: "Malnutrition causes Tuberculosis" ?]
Apart from the ones I've already mentioned, most of these quotes contain pretty accurate information.
Have you even looked beyond the title of this paper? If you did you would find that the authors do say microvesicles are contaminants and co-localisation can causes problems in centifuged virus preps, but they go to great lengths to unambiguously and unequivocally show that these are easily distinguished from HIV virions by way of their surface markers and HLA alleles. This paper is often cited by denialists who don't comprehend this point - you have merely shown yourself to be their equal in this regard. Bess' group have demonstrated the same phenomenon. The point of these papers is to show that contamination or "co-purification" is common, but that one can also readlily distinguish virions from microvesicles. What a shame - will you have to stop citing these papers in future, since they don't show what you think they do? (Somehow I doubt it - you'll just go on misquoting and misrepresenting them as usual, in the hope that no-one listening to you bothers to read the text of the paper and find they have been deliberately misled).
Andrew wrote:
"Wrong. A (highly invasive and metastatic melanoma cells) placed into the developing neural creast of an embryo) lead to the formation of normal dorsal root ganglia and other tissues)."
So, does this show that Duesberg's ideas about aneuploidy and cancer are insane? Do these metastatic invasive tumor cells not have gross chromosomal changes? Or do those chromosomal changes revert to normal? Has this work been published anywhere?
"... these are easily distinguished from HIV virions by way of their surface markers and HLA alleles."
DT, what about the "HIV virions" that CONTAIN HLA alleles at the surface?
Eugene Semon didn't understand what DT wrote or didn't read the paper. Probably both. Being an undergrad in Duesberg's lab is very time consuming so maybe we can forgive him.
The authors said HLA-DQ was found only in microvesicles based on their previous paper from 1997. HLA-DR is on virions and ratios change in infection. They also say CD43 and CD63 are "primarily virion-associated."
Point is, virions contain surface markers and probably other cell proteins in a way you can't explain by simple random distribution. Looks like they select some and exclude other ones.
Nice job though to Eugene, branching out from his usual HIV is an endogenous retrovirus.
The issue, Adele, is not that virions and vesicles are indistinguishable. They obviously are. The issue is the one of "purification". No PhD candidate has ever prepared an erlenmeyer flask containing only HIV virus particles with their little central cones, excluding impurities such as vesicles, other cell components and proteins. ALL the HV EM's show HIV virions placed over a background of cellular material.
Andrew,
After a number of people on this thread have pointed out that your arguments against the role of HIV in AIDS are entirely based upon distorting the work of other scientists by fabricating "quotes" or taking quotes out of context, you decide you no longer want to play "point-counterpoint".
What a surprise.
As far as "The ABC's of AIDS Denialism" piece goes, it seems to me that all you accomplished was to demonstrate the intellectual bankruptcy of your position.
No PhD candidate has ever prepared an erlenmeyer flask containing only HIV virus particles with their little central cones, excluding impurities such as vesicles, other cell components and proteins.
No internet troll has ever managed to construct a sentence containing 100% stupidity excluding any imputities of wisdom or intelligence. You come close though.
dear franklin,
perhaps you could show the readership a link to an EM HIV photo that shows HIV causing host cell damage. So far, none has been provided unless you consider the 1988 PNAS paper co-authored by Bob Gallo which showed cell damage upon release of HIV particles. Of course, we know this was a fabrication in 1988, and was later disproved.
Regarding the ABC's of AIDS denialism, there were about a 100 points made, and only one of them was actually found to be mistaken, and 99% is a fairly good batting average. Care to comment on the other 99 points that are completely valid?
Or, perhaps you would like to repeat your little mistake that Ariel Glaser never received IV AZT?
Ad hominems again, my noble doctor noble? Just address the question, and people will idolize you for the low life drug peddler you really are.
Thanks for the complement above. So this blog exercise has been useful to you also after all. I believe blogs like Tara's here are places to "air out" different sides of an argument-especially arguments as heated as ours regarding "HIV" and "AIDS," before putting anything into the peer-reviewed literature.
Your "treatise" has been on the internet for about a year. It might have been responsible and ethical to submit it to peer-review before you released it to the public.
The sad fact is that none of your target audience bothered to read the references and understand them enough to see whether they support your claims. They like to think they are skeptics but they aren't. They are just looking for someone to reinforce their existing beliefs.
The DAIDS 1997 official "HIV" culturing manual, under quality control, Section VI, page 45, advocates, "Do not use PHA stimulated PBMC older than 3 days post stimulation" when testing them for the absence of "HIV" from your healthy donor source.
It says point blank do not use PHA stimulated PBMCs older than 3 days. This includes for culturing HIV. The reason is simple if you se old preparations of PBMCs you may get false negatives.
Why not? Isn't it important to treat control cultures exactly the same in both duration and in what is added (PHA,etc.) in order to come to any conclusion about the experimentals?
It says to treat control cultures in exactly the same way. You should consider the possibility that you are deluding yourself into reading something that isn't there. Do you really think that the rest of the world is as stupid as you imply?
Ad hominems again, my noble doctor noble? Just address the question, and people will idolize you for the low life drug peddler you really are.
Amazing how you manage to still misunderstand the ad hominem fallacy.
I was attacking your argument. Insisting on an Erlenmeyer falsk full of 100% pure HIV is breathtakingly stupid. It is the last example of an endless series of goalpost moves that have long ago left the realms of science and moved to the heights of surrealist fantasy.
Nobody has ever purified stupidity to your standards. I'm pretty sure it exists though.
On the other hand accusing me of being a drug pusher is an example of the ad hominem fallacy.
My noble doctor noble, there are about a hundred points mentioned in the ABC's of Denialism. One was mistaken. A 99% batting average isnt bad. Instead of engaging in mental masturbation, perhaps you are forgetting the other 99 are pefectly valid.
By the way, we are still waiting for the link to the EM micrograph showing tagged HIV particles causing host cell damage. So far we have been given the old trick; "here's a list of 100 references, its in there somewhere", or an old 1988 Gallo PNAS article that was disproven.
It is starting to look suspicious Noble doctor noble, that you can't deliver. Might as well just admit it and come clean, there ain't none, my noble drug peddler, cause HIV doesnt cause cell damage in vivo. Professor Peter Duesberg was right in 1987, HIV is a benign pasenger virus.
Dont you agree?
kinda shy little bugger in vitro as well unless 'stimulated' in various ingenious ways.
My noble doctor noble, there are about a hundred points mentioned in the ABC's of Denialism. One was mistaken. A 99% batting average isnt bad. Instead of engaging in mental masturbation, perhaps you are forgetting the other 99 are pefectly valid.
You're not paying attention. We've already gone through several of the other points and found that he has been misquoting or misrepresenting the studies.
Laurent-Crawford, A. G., Krust, B., Muller, S., Rivière, Y., Rey-Cuillé, M.-A., Béhet, J.-M., Montagnier, L. & Hovanessian, A. G., "The Cytopathic Effect of HIV is Associated with Apoptosis", Virol. 185:829-839, 1991.
DAIDS official "HIV" culturing manual, under quality control, Section VI, page 45, 1997.
Horwitz MS, Boyce-Jacino MT, Faras AJ. "Novel human endogenous sequences related to human immunodeficiency virus type 1", J Virol. Apr;66(4):2170-9, 1992.
Abbott Package HIV-I ELISA Test Kit insert, 1997.
Epitope Package HIV-I Western Blot Test Kit insert, 1997.
Roche's amplicor HIV-1 monitor test, 1996.
"The Transfusion Safety Study Group", J Acquir Immune Defic Syndr; 5 (9):872, 1992.
Stramer et. al. "Detection of HIV-1 and HCV Infections among Antibody-Negative Blood Donors by Nucleic Acid-Amplification Testing", New England Journal of Medicine, Volume 351:760-768; August 19, Number 8, 2004.
If you really want I can go through some more. So far Maniotis has misquoted or misrepresented close to 100% of the referneces I have looked up. How many have you looked up?
Pilcher et al., "Detection of Acute Infections during HIV Testing in North Carolina", The New England Journal of Medicine, Volume 352:1873-1883, Number 18, May 5, 2005:
Firstly Pilcher et al use the term "at risk" not "high risk". They define "at risk" as "the population of persons who did not report a previous positive HIV test". Maniotis substitutes "high risk" for "at risk" and hopes nobody notices.
The other thing that staggers belief is what Maniotis fails to report from the study.
Out of the the 25 people that were HIV antibody negative and HIV RNA positive 2 later tested negative on RNA and antibody tests and 23 were confirmed to be infected with HIV. The RNA tests were highly specific and contrary to "rethinker" claims nobody is diagnosed as being HIV positive based on a single RNA test.
I believe he (Maniotis) makes some dubious claims about his own research in there as well. Something about HIV integrase not existing or some such...
dear noble doctor noble, this is just another typical tactic you guys use all the time. Making up games in order to avoid addressing the issues raised. We already discusssed the quote and the meaning of it ad nauseum for this reference, you and your associates demonstrated your robotic abilities to scan the text without comprehension of it. Out of 37 million tests, there were 12 HIV RNA pos, HIV AB neg because of window period, remember? This is AIDS Denialism because 12 acute window infections are not enough to maintain a milion a year. You may disagree or agree, but it is perfectly valid. and the others are similar, you guys have no reading coprehension. Try an evelyn woods speed reading course.
Stramer et. al. "Detection of HIV-1 and HCV Infections among Antibody-Negative Blood Donors by Nucleic Acid-Amplification Testing", New England Journal of Medicine, Volume 351:760-768; August 19, Number 8, 2004.
dear noble doctor noble, this is just another typical tactic you guys use all the time. Making up games in order to avoid addressing the issues raised. We already discusssed the quote and the meaning of it ad nauseum for this reference, you and your associates demonstrated your robotic abilities to scan the text without comprehension of it. Out of 37 million tests, there were 12 HIV RNA pos, HIV AB neg because of window period, remember? This is AIDS Denialism because 12 acute window infections are not enough to maintain a milion a year. You may disagree or agree, but it is perfectly valid. and the others are similar, you guys have no reading coprehension. Try an evelyn woods speed reading course.
Yes, we've already been over this.
Maniotis substituted "non-risk" for "HIV antibody negative". An accident? I don't think so. The quote was not verbatim.
Maniotis also fails to tell his audience that blood donors are required to fill out a Blood Donor History Questionnaire before they can give blood.
Expecting the number of acute HIV infections detected in donated blood to be representative of the total population is simply stupid. That rasises the question of who exactly maniotis is trying to fool. You can answer that better than me.
The noble doctor noble says
Yes, we've already been over this. Maniotis substituted "non-risk" for "HIV antibody negative". An accident? I don't think so. The quote was not verbatim.
I reviewed the quote and it was correct. When you quote word fragments, it looks like you are trying yourself to be deceptive.
Maniotis also fails to tell his audience that blood donors are required to fill out a Blood Donor History Questionnaire before they can give blood.
So what? Window infections dont show up on a questionnairre.
This is the height of lunacy. Everybody knows about the questionarre. Even high school kids know about it. You are hilarious.
Expecting the number of acute HIV infections detected in donated blood to be representative of the total population is simply stupid. That rasises the question of who exactly maniotis is trying to fool. You can answer that better than me.
It may seem stupid to you, are you stupid? You have no reference to support your claim. Who are you trying to fool? A link to a blood bank questionnaire does not support your claim that 12 window infections detected in 37 million tests of donated blood is enough to maintain 1 million infections per year in the population of blood donors. There are 40,000 blood donations a day in America. Where do you think the blood is coming from? The Chinese? Its coming from Americans. Don't forget, window infections will not show up on a questionnaire and will not show up on HIV antibody tests. There is major marketing going on to induce people, all people, to donate blood.
From a blood bank site; "the greatest barrier that prevents people from donating is a lack of convenience and a lack of knowledge of the importance of donating, experts say. And it is important. Every pint of donated blood saves three lives, and someone needs blood every three seconds."
You are pathetic.
It may seem stupid to you, are you stupid? You have no reference to support your claim. Who are you trying to fool? A link to a blood bank questionnaire does not support your claim that 12 window infections detected in 37 million tests of donated blood is enough to maintain 1 million infections per year in the population of blood donors. There are 40,000 blood donations a day in America. Where do you think the blood is coming from? The Chinese? Its coming from Americans. Don't forget, window infections will not show up on a questionnaire and will not show up on HIV antibody tests. There is major marketing going on to induce people, all people, to donate blood.
There aren't one million infections per year in the US. The estimate is about 40,000 infections per year.
If you had bothered to read the questionnaire then you would have noticed that they ask you whether you have had sex with people that are HIV+, prostitutes, people with haemophilia etc
People at high risk of being infected with HIV are effectively screened
from donating blood.
There is major marketing going on to induce people, all people, to donate blood.
Blood Donation Frequently Asked Questions
There aren't one million infections per year in the US. The estimate is about 40,000 infections per year.
Wait a minute, there's a million people with HIV annually, right? All HIV die of AIDS, right? So, that means there HAS to be a million new infections to replace the million who die of AIDS. Since you claim there are ony 40,000. You, my noble doctor noble, are an AIDS DENIALIST.
If you had bothered to read the questionnaire then you would have noticed that they ask you whether you have had sex with people that are HIV+, prostitutes, people with haemophilia etc.
What about the heterosexal AIDS epidemic penetrating into the general well-to-do population? Are you telling me thats a lie, too? Again my noble docotr noble, you are an AIDS DENIALIST.
People at high risk of being infected with HIV are effectively screened from donating blood.
Are you telling me that "low risk" people can't and don't get HIV by virtue of their color or socio-economic status? Either the HIV bug has brain function to use racial discrimination, or you, my noble doctor noble, are a racist, and an AIDS DENIALIST.
My noble doctor noble, you are ignoring the fact that, one percent of the blood is discarded because of positive serology. If your questionnare is so good at screening out HIV, then why are 37 million tainted blood donations discarded every year? Your clean blood donors are not so clean, even with the questionnaire, which by the way is not a reference in the medical literature to support your claim. You have no claim my noble doctor noble except for the dogma your masters fed you, my little sock puppet.
By the way, your sock puppet troll, Roy Hinkley, alias Nick Bennett, cited a 1988 PNAS Gallo paper figure 4, EM of cell damage after HIV particle release. This was found to be another Gallo lie in the medical literature contradicted by 19 years of EM research from 1988 to 2007.
What about that my noble doctor noble? Cat got your tongue? Still no link to the page showing EM of HIV producing host cell damage. We are waiting. The silence is deafening, my little sock puppet.
Dear Black Falcon / forty mules / Patriot games ....
Please look up the difference between prevalence of a condition and incidence of a condition. You plainly do not know. Until you do, I suggest you shut up and stop embarrassing yourself.
Please look up the definition of "sock puppet". You plainly do not know. Until you do I suggest you stop accusing others of being one. Dr Noble has never resorted to puppetry, but you have very frequently.
I don't know why Noble continues to make a fool of himself. It is common knowledge that Black Falcon is correct. Everyone knows that exactly one million people in the USA die of AIDS every year, and Duesberg has shown that the number of currently infected people is always exactly one million since 1984. So there must be one million new infections ever year to replace the one million that die.
As soon as anyone tests HIV-positive they are put on AZT and die within 6 weeks. That is how our graveyards filled up with the 23 million AIDS deaths that have occurred between 1984 and 2007. It is iatrogenic, all of these 23 million people would be alive today without AZT.
White Parrot - I think you need to insert a smiley after your post.
The denialists on line here are too intellectually challenged to appreciate your irony. Even Maniotis does not have to misquote you!
Black Falcon wrote why are 37 million tainted blood donations discarded every year?
Now there's a statistic for you! I wonder where it came from ...
Dale said:
Black Falcon wrote why are 37 million tainted blood donations discarded every year?
Now there's a statistic for you! I wonder where it came from ...
Very funny. Yes there is a correction here, its 1 per cent of total donations of 37 million anually or 37 thousand discards annually. Thanks for pointing out the decimal point error. The meaning and content of the comment remains the same however.
I admit my mistake with honor and pride, unlike your associates, the low life political AIDS activists and drug company sock puppets who haven't given a link to a single EM photo of HIV damaging the host cell. What a bunch of losers. All they do is mentally jerk around with their nit picking robot comments. There is no evidence that any of them has ever had an original thought.
Duesberg was right back in his classic 1987 book, "Inventing the Aids Virus", HIV is a benign passenger virus and does NOT damage its host cell.
The silence is deafening.
Yes there is a correction here, its 1 per cent of total donations of 37 million anually or 370 thousand discards annually.
Again you're wrong Gray Crow. Donations in the United States reached 15 million in 2001 because of 9-11 and that's about the highest they ever get. Discarded blood is around 200,000 units per year. So 1 to 2 percent gets discarded.
Blood gets discarded for alot of reasons. Iron is a big one. Age might be the top one, blood's been around too long. There's tests for autoantibodies. Another big one is positive on the RPR for syphilis and if you want to talk false positives, that's false positive alot with RPR unlike HIV tests. And more. So most of the reasons for discarding blood aren't things people know about unlike risk behavior for the STDs.
Blood donors are usually really conscientious people who are trying to help out. They don't usually lie about a condition they know they have. If they do, their tagged and they can never donate again.
Black Falcon, everything you say is BS. Nothing personal. Just how it is.
Everyone knows that exactly one million people in the USA die of AIDS every year, and Duesberg has shown that the number of currently infected people is always exactly one million since 1984. So there must be one million new infections ever year to replace the one million that die.
Everyone knows the virus is 100% deadly given time, so one would expect after 23 years, which is the official current life expectancy if one adheres religiously to the life saving drugs, that AIDS incidence would kinda, sorta have gotten closer to HIV incidence than 40,000 to 1,000000 or what?
That HIV prevalence, not incidence
Huh?
You betcha Mr. President.
The Black Falcon asked me to thank you adele for that very erudite BS comment. By the way, Adele, where's the link to the EM photo showing HIV induced host cell damage? Talking of BS, Adele, you get the prize. There are no EM photos of HIV induced host cell damage because HIV doesn't damage the host cell. Why not come clean Adele, and admit this obvious fact? Duesberg was right from the beginning in his 1987 book, Inventing the Aids Virus. Adele, we know you have knowledge of the EM literature. This should have been posted in 30 seconds for all to see. What's the problem? Afraid the sponsors will pull the plug because Duesberg was right? and Aetiology becomes just another AIDS denialist web site? This is 2007 Adele, not 1984, and although you can fool some of the people some of the time, can't fool anyone anymore. The jig is up. Every one knows by now.
Since you aren't familiar with EM I'll explain this to you. Oh and Duesbergs book was published 1996 not 1987.
EMs of cells death, this is like saying after you run a red light and crash, "do you have pictures of my automobile accident taken from the Hubble Telescope? Well then obviously I didn't cause it."
The Hubble Telescope is a kind of expensive specialized thing to use for traffic survellance. When you've got a traffic cam and ten witnesses you don't need a picture from the Hubble. If you asked for it in court you're just showing how desperate your case is and they'd rule you at fault.
Same with EMs for cell damage. Yeah, you could see some cell damage with EMs but who uses them this way. HIV kills cells and theres a bunch of ways to test this biochemical using a light scope etc. They're all faster and easier than a EM. When you insist on having EMs of HIV killing cells, you just demonstrate you don't understand what an EM does or what HIV is or well you just show how much you need to learn to sound like you know what your talking about. Could we find some papers or some unpublished images that outnumber the published ones like a hundred to one by the way that show something like this, maybe, but I don't have the time to do that for someone who can't do the research for his bird-brained self. And who's going to raise the bar again anyway once he has what he pretends he wants.
Bespotted parrot; no virus is 100% deadly. The rabies virus is very close, but even a couple of people have now survived untreated infection with rabies. HIV was never said to kill 100% of infected individuals. Only the denialists have used the HIV=AIDS=Death statement, claiming that the "orthodoxy" has said this.
Where did you read that the "official life expectancy" for HIV infection treated with HAART is 23 years? Many papers now state that with adequate treatment, HIV-infected people can expect to live very nearly normal lifespans. See for example:
Lohse N, Hansen AB, Gerstoft J, Obel N.
Improved survival in HIV-infected persons: consequences and perspectives.
J Antimicrob Chemother. 2007 Jul 2; [Epub ahead of print]
PMID: 17609196
Cohen CJ.
Successful HIV treatment: lessons learned.
J Manag Care Pharm. 2006 Sep;12(7 Suppl B):S6-11.
PMID: 16984222
Piacenti FJ.
An update and review of antiretroviral therapy.
Pharmacotherapy. 2006 Aug;26(8):1111-33. Review.
PMID: 16863488
Black Falcon posted who haven't given a link to a single EM photo of HIV damaging the host cell.
I see Adele beat me to it but I too am curious about this preoccupation with EM photos. What in your opinion would an EM tell you about the ability of HIV to damage cells that any one of a number of biochemical assays wouldn't tell you more cheaply and, in my opinion anyway, more convincingly?
Bespotted parrot; no virus is 100% deadly. The rabies virus is very close, but even a couple of people have now survived untreated infection with rabies. HIV was never said to kill 100% of infected individuals. Only the denialists have used the HIV=AIDS=Death statement, claiming that the "orthodoxy"
Oh is that so, dr? Well, I don't want to make it too difficult for you, so for argument's sake let's agree.
Jefferys and Dr. Noble are the ones who told me there are between 1.5 and 5% LTNPs. I'll generously let you take 5% off the top of HIV prevalence numbers the last 25 years. Now explain the 40,000 AIDS case incidence compared with 1,000000 HIV prevalence.
The 23/24 years for wealthy ARV addicts I get here: http://www.foxnews.com/story/0,2933,228798,00.html
Note "A 1993 estimate of life expectancy for a symptomless person infected with HIV was less than seven years".
Bespotted Parrot; assuming the figure of one million HIV-infected people is correct; and that it has been ten years since HAART became available to raise life expectancy to 24 years post-treatment, we have to wait another 14 years for the people who began treatment ten years ago to die. The few thousand HIV-iunfected people who will die this year, are those on the wrong end of the bell curve, not those at the peak of it.
I don't get what this birdy is asking. Maybe he should just go watch Fox or maybe listen to Rush some more.
Estimated 40,000 new infections in the United States every year. Less than 20,000 AIDS deaths per year, maybe around 20,000 since some underreporting happens. More people are infected with HIV every year but the growth isn't as fast as a few decades ago. By discovery of AIDS it was maybe half a million infections. Today between one and two million.
Of course the patriotic denial parrots crows falcons ducks and other feathery friends say its always been a million exactly on the nose plus or minus three people from Christopher Columbus to today and then until their LORD AND SAVIOR Phyllis Schlafly returns in the clouds someday. I mean who would you believe? Epidemiologists who study this stuff all the time or Peter Duesberg who fudged some other peoples numbers in his crappy reviews?
dr,
Since the life expectancy estimates are constantly revised 1. as sales argument for the drugs 2. to explain why people aren't dying when they're supposed to, you are free to assume all you want. That's why I added that little tidbit of information from the Fox News story:
Note "A 1993 estimate of life expectancy for a symptomless person infected with HIV was less than seven years"
Now again make that 9-10 years if you want, go to '95 and tell me where are the graves of the close to 1,000000 HIV+ from 1985-86 who had by then used up their life expectancy.
Bespotted Parrot, there were not a million people infected with HIV-1 in the USA in 1984 or 1985. HIV-1 only entered the USA in the late 1970s. Before the gay community knew to start practicing safe sex and the IV drug users were counseled to stop sharing needles (around 1982, when it became obvious that GRID or AIDS was a transmissible disease and not a "lifestyle" or chemical type of problem), the number of infected people grew very rapidly to tens of thousands. However, once it was clear that this was a sexually transmitted (and blood borne) pathogen, the bath houses were closed etc. and the rate of growth of the epidemic slowed dramatically. Even before HIV tests were available to screen the blood supply, measures were put in place to restrict donations by high risk individuals, so even transfusion mediated infections slowed a bit before 1985.
Laverdiere M, Tremblay J, Lavallee R, Bonny Y, Lacombe M, Boileau J, Lachapelle J, Lamoureux C.
AIDS in Haitian immigrants and in a Caucasian woman closely associated with Haitians.
Can Med Assoc J. 1983 Dec 1;129(11):1209-12.
PMID: 6640458
Centers for Disease Control (CDC).
Prevention of acquired immune deficiency syndrome (AIDS): report of inter-agency recommendations.
MMWR Morb Mortal Wkly Rep. 1983 Mar 4;32(8):101-3.
PMID: 6403825
Griffin JP.
Acquired immune deficiency syndrome: a new epidemic.
Crit Care Nurse. 1983 Mar-Apr;3(2):21-4, 28.
PMID: 6301753
Valle SL, Ranki A, Repo H, Suni J, Ponka A, Lahdevirta J, Pettersson T.
Acquired immune deficiency syndrome. The first cases in Finland.
Ann Clin Res. 1983;15(5-6):203-5.
PMID: 6607697
Oleske JM, Minnefor AB.
Acquired immune deficiency syndrome in children.
Pediatr Infect Dis. 1983 Mar-Apr;2(2):85-6.
PMID: 6856494
Francis DP, Curran JW, Essex M.
Epidemic acquired immune deficiency syndrome: epidemiologic evidence for a transmissible agent.
J Natl Cancer Inst. 1983 Jul;71(1):1-4.
PMID: 6575197
dr said, there were not a million people infected with HIV-1 in the USA in 1984 or 1985.
Which of your references, if any, support this statment with data?
Where are your references that 1 million WERE infected in 1984?
Just Duesberg, who lied about his sources.
There were about 450,000 give or take a few infected in 1984 in the United States.
Weirdly, Gray Crow, you didn't even have time to read ANY of dr's sources before you commented.
"The DAIDS 1997 official "HIV" culturing manual, under quality control, Section VI, page 45, advocates, "Do not use PHA stimulated PBMC older than 3 days post stimulation" when testing them for the absence of "HIV" from your healthy donor source.
Chris: "It says point blank do not use PHA stimulated PBMCs older than 3 days. This includes for culturing HIV. The reason is simple if you se old preparations of PBMCs you may get false negatives.
"Why not? Isn't it important to treat control cultures exactly the same in both duration and in what is added (PHA,etc.) in order to come to any conclusion about the experimentals?
Chris: "It says to treat control cultures in exactly the same way. You should consider the possibility that you are deluding yourself into reading something that isn't there. Do you really think that the rest of the world is as stupid as you imply?
The above point-counterpoint shows how desparate Chris has become in his attacks on Dr Maniotis.
In his first response, the point is precisely backward if you read the entire 10 page section of the manual since it's terminating too soon that can produce a false negative.
Dr Maniotis has indeed drawn an inference as far as a suitable control being defined out of the procedure by a "quality control" statement.
Adele, I was talking about '85-'86. dr changed it to '84-85, and all his referecnes are from '83. HWy don't you go read them and see if the CDC back-calsulations fro '86 are found in any of them?
Hi Nick,
This is cut-n-pasted from above:
On the remote chance that you are genuinely confused and not just being disingenuous, let me spell it out for you.
Control cultures are treated exactly the same in both duration and in what is added.
In order to expand a population of HIV in culture, you need to supply the culture with fresh potentially infectable T cells at regular intervals. (In vivo those fresh potentially infectable T cells are entering the peripheral blood from the lymph nodes etc. ) In vitro they are supplied as PBMC from an non infected source that have been PHA stimulated for no more than 3 days.
So control cultures or HIV infected cultures are 'fed' every 3-4 days with some PHA stimulated PBMC from a non infected source.
Dear Dr. Duke, and Adele
Andrew wrote:
"Wrong. A (highly invasive and metastatic melanoma cells) placed into the developing neural creast of an embryo) lead to the formation of normal dorsal root ganglia and other tissues)."
"So, does this show that Duesberg's ideas about aneuploidy and cancer are insane? Do these metastatic invasive tumor cells not have gross chromosomal changes? Or do those chromosomal changes revert to normal? Has this work been published anywhere?"
Posted by: Dr. Duke | July 5, 2007 02:57 PM
Peter's ideas regarding aneuploidy aren't insane. I believe our data show, unlike the data of Peter and others which were derived from 2-dimensional tissue-culture plastic dish bottom cultures, that cancer can be controlled epigenetically, and that aneuploidy does not drive cancer, and is not specific to cancer, but is controllable by the extracellar matrix environment of a cell. But this is not a new idea: Barbara McClintock's variegated leaves is only possible through her observations of the chromatin-bridge-fusion cycle and consequent resulting aneuploidy in the differentiated leaves, and Boveri's diminution in normal Ascarid development of somatic cells is only possible through kicking out chromosomes at each successive division, while germ line chromosomes all remain in these cells as an intact euploid set (so inheritance will proceed with all the necessary worm genes). Because normal differentiation phenomenon such as leaf variegated leaves described by McClintock and Ascarid diminution described by Boveri aren't cancer in either plants or animals, aneuploidy is not specific for cancer but plays an important role in normal development (as well).
It took 20 years to convincingly develop this idea using modern experimental biological techniques to a point where the scientific community accepts this idea as being correct. For instance, the idea was brewing in the laboratories of Mina Bissell, Judah Folkman, and several others when I worked as a lab tech in 1985 (and where I first met Peter Duesberg). One day, using control cultures on special 3D matrices I engineered without neurons, luck smiled on us and we observed that all of the morphological features and molecular expression of neonatal, and partially adult muscle histogenesis in 3D in vitro cultures (Strohman, R.C., Bayne, E., Spector,D., Obinata,T., Micou-Eastwood, J., Maniotis A. Myogenesis and histogenesis of skeletal muscle on flexible membranes. In Vitro Cell Dev. Biology, Vol 26: pp. 201-208, 1990). At The University of Iowa (a place I loved and which is the reason I decided to spend some time with Tara's blogs with the hopes that we could get some discussion going after years of censorship), some years later, luck smiled on us again when we were the first to demonstrate tissue patterning, and molecular construction of melanomas that resembled and functioned in many ways like real melanomas in patients (Maniotis A., Folberg R., Hess A., Seftor E., Gardner L., Pe'er J., Trent J., Meltzer P., Hendrix M. Vascular channel formation by human uveal melanoma cells in vivo and in vitro: Vasculogenic mimicry. Amer. J. Path. Vol. I55, No 3, pps. 739-752, September, 1999). Only recently, with the help of a very talented postdoc has it happened that, and because of a growing acceptance of epigenetics in cancer, that a journal has asked ME if they could put our work on the cover as they did in this May issue of The American Journal of Pathology, with the hard won 3 letters, 'Epi' preceding the words-genetic reversion of breast cancer DNA (Tone Sandal, Klara Valyi-Nagy, Robert Folberg, Mina Bissell, Virginia Spensor, Andrew Maniotis. Epigenetic reversion of breast carcinoma phenotype and DNA sequestration. American Journal Of Pathology, Vol. 170(5):1739-49. May, 2007).
Moreover, we have been fortunate enough to employ new global genomic approaches to testing DNA in both normal and cancer cells, and show how breast cancer morphology, tissue organization, and DNA are epigenetically revertible in melanomas and breast cancers by using single extracellular matrix molecules such as laminin and fibronectin.
When Peter published his beautiful 1997 PNAS paper on aneuploidy being present in 100% of chemically induced CHO-cell transformations in vitro, we begin at that time to analyze cancer genomics in melanoma with great intensity, in order to test the null hypothesis: that for every tumor, if aneuploidy is correct and drives progression, then every tumor (every patient's melanoma) should have a different genotype, if not a different karyology. However, at the chromosomal level, there appears to be regular aneuploidies occurring (check out the work of Bill Harbour at Washington University for example), and these regular aneuploidies appear to correlate with progression in melanoma at least. Therefore, one can only be resigned to the fact at this point that McClintock's and Boveri's aneuploidy phenomenon are a larger issue associated with both normal differentiation and cancer. Our breast cancer reversion work suggests that aneuploidy does not in any way drive cancer, but instead, is controlled from the outside of cells by the extracellular matrix microenvironment in regular, predictable ways, that hopefully in time, will translate into an understanding of how regular patterns of aneuploidy may be present in certain tumor types, or regular sub-chromatin-organizational features of chromatin (such as methylation) is regular and can be predicted.
On the other hand, so far, in malanoma, I have found nothing to invalidate the hypothesis that DNA is indeed globally altered in all cancers through the sequestration and exposure of thousands of genes by disulfide-rich proteins as we reported a few years ago after extensive microarray analyses, in conjuction with tissue culture validation and validation in human tumors compared to their normal marginal tissue (Maniotis AJ, Valyi-Nagy K, Karavitis J, Moses J, Boddipali V, Wang Y, Nuñez R, Setty S, Arbieva Z, Bissell MJ, and Folberg R: Chromatin organization measured by Alu I restriction enzyme changes with malignancy and is regulated by the extracellular matrix and the cytoskeleton. Am J Pathol 166: No. 4 April 2005). These observations are consistent with the aneuploidy being ASSOCIATED with cancer progression but not causal for progression, compared to the influence of the microenvironment. Nor we reliably predict if a melanoma will kill or not, based on its degree of aneuploidy, but can predict patient outcome based on a tumor's cell's degree of DNA sequestration, and as we originally established, by the detection of vasculogenic mimicry (see reference above). To date, for instance, we have found wildly aneuploid cells in melanomas with 3N or all over the ploidy map that are in no way invasive. By contrast, we have found highly invasive and metastatic melanomas with a chromosomal complement that is near euploid. The changes that are important are occurring globally indeed at the level of chromatin, but not necessarily with ploidy, but at the level of the disulfide bond-rich proteins in the nuclear matrix.
One conceptual framework that has attempted to explain the complexities of neoplasia is an ontologically based idea: Waddington and Needham first suggested that cancer occurs because of a breakdown of what he termed "individuation fields" that are set up early in development and which normally persist throughout life (Waddington CH. Cancer and the theory of organizers. Nature 1935, April 20, 606-608; Needham J. New advances in the chemistry and biology of organized growth. Proc. rol. Soc. 1936 B. 29 1577-1626.
That such so-called individuation fields may exist is given credence by reviewing the findings of classic tissue transplantation experiments performed by such investigators as Rose and Wallingford, (Rose MS. Wallingford H. Transformation of renal tumors of frogs to normal tissues in regenerating limbs of salamanders. Science 1948 May 6, Vol 107, 457), and others. The common theme of these tumor cell transplantation experiments into embryonic fields involves the placement of malignant cells (or cancer inducers) specifically into biological contexts that are actively developing and demonstrating reversal of tumor cell properties, or a reverse transformation of the tumor cells into normal cells or tissues. Teratocarcinoma that kill adult mice, when placed into developing blastulas, do not induce cancer after blastula formation, in the adult organisms that form, or even if some of the cells become incorporated into the developing germ line lineage, the offspring remain cancer-free. (Illmensee K, Mintz B. Totipotency and normal differentiation of single teratocarcinoma cells cloned by injection into blastocysts. Proc Natl Acad Sci U S A 1976;73:549-553) .Highly invasive and metastatic melanoma cells derived from a human liver metastasis will form normal dorsal root ganglia when placed in the developing neural crest of the bird embryo. (Kulesa PM, Kasemeier-Kulesa JC, Teddy JM, et al. Reprogramming metastatic melanoma cells to assume a neural crest cell-like phenotype in an embryonic microenvironment. Proc Natl Acad Sci U S A 2006;103: 3752-3757).Organisms that do not have vital centralized organs such as tobacco plants, but which develop cancers, show that the malignant properties of Crown Gall tumor cells can be reversed through serial transplantation to cut and growing stems. (Braun AC. The cancer problem: A critical analysis and modern synthesis. Columbia University Press New York and London 1969). The lesson is to see how nature can reverse a disease process and perhaps augment or apply it to a situation to reverse disease. Cancer is contextual-it varies depending on the primary site, the type of cancer, the age of the cancer patient, and nobody can assume to treat 2 patients the same way who has ever dealt with the disease. But you want to round up millions of people by force if necessary (most of whom are Black or gay), lump 47 previously known "AIDS-indicator diseases" into a single category, and subject them to toxic and dangerous pharmaceutical or vaccination approaches, although profound immunosuppression is caused by a myriad of factors?
But viruses, and culturing them are problematic. In vitro, viruses behave completely differently depending on whether they are cultured physiologically in a 3D matrix or whether they are grown artificially in flat dishes that contain media (instead of 100% human serum for instance (Klara Valyi-Nagy, Robert Folberg, Tibor Valyi-Nagy, Andrew J. Maniotis. Susceptibility of Herpes simplex Virus Type I and II, The Role of Tumor Invasiveness, The Extracellular Matrix, and Chromatin Sequestration. In press, May, Experimental Eye Research, Vol. 84, 9991-10,000, 2007).
In terms of cause and effect, and as I have I believe adequately posted above, the association of viruses and cells create problems because the viruses must depend on the cell constituents for all of their materials. In terms of viruses and cancer, it is doubly problematical, because as I have stated on http://www.ddponline.org/vande.htm, it is nothing less than Nazi-like human experimentation at this point in our understanding of viruses, to experiment on hundred of millions of people with contaminated vaccines like the polio vaccines, where in retrospect it was admitted that a contaminant transforming virus, SV-40 that found its way into the vaccine from infected monkey kidney cells supposedly caused all kinds of mesotheliomas in rodents and other animals, and then to ignore the evidence in controlled trials that even in this greatest blunder of the 20th century showed, that there is no evidence that this cancer-causing SV-40 could cause cancer in humans (the evidence is much much weaker for a link between viruses and cancer with HPV, HBV, HCV, HTLV-1 than this massive human polio study). For example, even in the 35 year post-polio vaccine mortality studies, initiated because the so called potent cancer-causing virus, SV-40 was inoculated into more than 100,000,000 Americans and twice as many Europeans and Soviets, along with the polio virus that increased the background incidence of polio in California 3 fold, in Idaho 15 fold, and in other places currently like Nigeria and India who have had massive 15 year polio campaigns some hundreds of fold), has not been long enough to determine if SV-40 is contributing to escalating cancer rates. The thirty-five year mortality study on people now in middle age following receipt of SV40-simian-(cancer) virus -contaminated polio vaccine show that out of 1073 newborns that were vaccinated and carefully followed for 35 years, (which the authors claim is not really long enough) of the 100,000,000 individuals or more that were given this "cancer virus-contaminated vaccine, " between 1959 and 1963, there has been no apparent increase in cancer above the expected background incidences in this carefully followed subgroup (Carroll-Pankhurst et al., British Journal of Cancer 85 (9) 1295-1297), although some would dispute this conclusion (especially in Australia).
This brings me to the DIADS culturing manual charges against me. Simply stated, the statement I quoted correctly:
The DAIDS 1997 official "HIV" culturing manual, under quality control, Section VI, page 45, advocates, "Do not use PHA stimulated PBMC older than 3 days post stimulation" when testing them for the absence of HIV from your healthy donor source,"
was taken out of context of the argument I was making because in
"The Reporting Results Section which follows (section VII) a rationale follows that obviously employs both healthy (or non-"infected" cells-although I don't think anybody tests intentionally non-"infected cells") in a manner that is irrational to my way of thinking, unless I really don't understand what is going on. For example:
If "cultures whose supernatant meet one of the following criteria are considered culture positive IF:
"Two consecutive HIV p24 antigen VQA CORRECTED values of > 30 pg/ml, of which the second value is at least four times greater than the first value or "out of range" (O.D.>2) or
"Two consecutive HIV p24 antigen VQA CORRECTED values that are "out of range (Optical density.> 2); or
"Three consecutive HIV p24 antigen VQA CORRECTED values of > 30 pg/ml, where neither consecutive value is > four times the previous sample, but the third value is at least four times greater than the first,"
then is a sample considered negative if two consecutive HIV p24 antigen VQA corrected values read > 25 pg/ml but < 28 pg/ml? Or is this considered the same or equivalent as would be a healthy donor source, regardless of whether or not it came from a 3 day pre-treated source of cells, a cervical smear, or the list of other sources provided in the beginning of the manual and regardless of which biotech vendor's antibody was used that litters the back half of the manual?
In other words, with two consecutive readings of 29 pg/ml, can I go out and party tonight and screw anybody I want without worrying that I would be tried along side Parenzee, or should I go blow my brains out (rather than let Marc Wainberg throw me in his AIDS ward or subject myself (or a child) to anti-retroviral diarrhea, wasting, heart disease, mutagenesis from the drugs, an inability to walk or even hold a pen as some HAART AIDS patients I know have described, because I now must take for the rest of my life the meds that John Moore said the other day is kind of difficult to sprinkle on my cornflakes cause "its kinda like cancer chemo for a serious disease," and which the AIDS establishment will never let me cease from taking (as oncologists ethically must do if they use the same class of drugs at the same dosages on terminal cancer patients)?
Its even more confusing given that p24 is found, according to at least one group, in the kidneys of non-HIV-infected children (Dura WT, Wozniewicz BM. (Expression of antigens homologous to human retrovirus molecules in normal and severely atrophic thymus. Thymus 22 (4):245-54, 1994).
What kind of culturing diagnostic technique is this? Especially when Gallo said in the Parenzee trial something as to the effect that (and this is not a direct quote you guys so don't get excited because I know you read the entire Paranzee manuscript also and will recognize it):
'Not one molecule of "HIV's" proteins would be present in a whole stadium full of sports fans, given none of them were HIV postive.'
Well gee Mr. Gallo, Mr. Fauci, Mr. Wainberg, I got 29 "units" of p24 in my blood, so I guess its safe that I can go after the cheerleaders or donate blood tomorrow! I ain't got 30 pg/ml on two consecutive tests, so I OK! For shame! I'd rather take my chance with phrenology as a test for intelligence, or burning witches to see if they die (as you did to Christine's family). But I'd bet that, naïve to the absolute junk science of the "HIV/AIDS" religion, and if somehow convinced to take an "HIV" test (or now under mandatory testing conditions at my "routine checkup" without any informed consent as is currently in place by the Nazi administration), that I'd finally fulfill Jesse Helm's dream-to be afraid of any cheerleaders, and to regard for sure selectively biased populations such as gays (and African Americans) as being the object of "God's revenge." How are you supposed to feel if you blew a 29 on an AIDS breathalizer p24 test?
The DIADS culturing manual, in light of the warnings of Larent-Crawford are even more disturbing, and suggest, if you really think about it, that not only are there no animal models of "HIV," but there are no in consistent vitro models either, despite the DIADS attempt to codify a single set of protocols for normal stimulated lymphocyte culturing coupled to a diagnostic that doesn't make any sense.
Most heartbreaking of all, perhaps, is the fact that the equation of p24, or the spate of other "hidden epitope antibody tests or phony nucleic acid testing described in the last half of the DIADS handbook, all suffer from the same problems that Bess et al., (1997) so eloquently described (Microvesicles are a source of contaminating cellular proteins found in PURIFIED HIV-1 preparations." In other words, on top of there being no consistent cell culturing model for "HIV's" so-called pathogenic effect (principally but not only due to the problems with mitogen interference that causes, according to Laurent-Crawford et al., unbalanced signals and apoptosis or syncytial formation or persistant non-pathogenic viral production depending on whether lymphocytes are "immature or "mature" there is still, no evidence whatsoever, that p24 has anything to do with an exogenous virus called "HIV." I'd like to give a few examples:
1. If you go to figure 3 in this paper, one cannot tell a piece of cellular debris from any other piece of debris or crap. And this is where p24 was isolated from under the best PURIFICATION conditions that "HIV" science could muster? If you want to see what a virus prep for purification should look like, see http://www.virusmyth.net/aids/news/edhlettercont.htm
And note that there isn't any crap that can co-purify and be mistaken for a unique, exogenous, viral protein, or at least its highly unlikely. The author points to the two pieces of shit in the prep that aren't viral in nature in a background of hundreds that are identical.
2. The authors specifically state that: "Identification and analysis of the virus are complicated by the presence of cellular membrane vesicles which COPURIFY with the virus."
3. "We recently reported a proteolytic procedure (Ott et al., 1995b) that effectively rejmoves greater than 95% of proteins associated with these membrane vesicles. This procedure has allowed us to demonstrate that the cytoskeletal proteins, actin, ezrin, moesin, and cofilin are located IN THE INTERIOR of virions."
Question: If actin, exrin, and cytoskeletal proteins are located INSIDE the virions, how can one tell if p24, which is a faint band on most cellular gels that come from non-infected cells in most labs, is also a cellular protein? The gel shown in figure 1 (the non-infected lane) has weaker bands at all of these weight designations that supposedly the infected supernatants were run (B,C). In fact the p24 band is extremely PRESENT in lane A, which is the uninfected lane. This gel is the basis for giving someone cancer chemo on their cornflakes for life? For shame!
4. "PHA activated human PBLs were also shown to produce microvesicles that incorporated cellular proteins (Fig. 6)."
5. "In addition to proteins, microvesicles (AND CENTRIOLES AND CELLULAR NUCLEI-MY INTERPRETATION) were also shown to contain both RNA and DNA. Approximately 10ug of RNA and 4 ug of DNA were found per mg of protein. The major RNA species in microvesicles were ribosomal 28S and 18S subuitis and some low molecular species, PERHAPS tRNA."
Could these nucleic acids form little dark "cones" one might ask? Hard to tell you say. Look at figure 3 and tell me in those several dark cone-containing pieces of cellular crap, do you see your father, the sea, Mana from heaven, the "HIV" genome, your future?
6. "We have been unsuccessful at separating microvesicles from HIV- by centrifugation techniques (data not shown)." What! It's shown in figure 3!
7. GP120 may do the trick (if it isn't a cellular protein which it is).
8. "Clearly, future experiments utilizing purified viruses must be carefully controlled to account for the effects of cellular antigens present on microvessels" (like p24 and all the other so-called proteins and nucleic acids thought to be specific to "HIV"). Clearly indeed!#@###$@
9. "Numerous other cellular proteins have been identified in PURIFIED preparations of HIV-1. It is not known if these are physically associated with HIV particles and, if so, whether or not they have a role in the virus replication cycle. IDENTIFICATION OF WHICH CELLULAR PROTEINS ARE ASSOCIATED WITH THE VIRUS IS A PREREQISITE TO STUDYING THE POTENTIAL FUNCITON OF CELLULAR PROTEINS IN THE VIRUS REPLICATION CYCLE."
SHOULD READ:
"IDENTIFICATION OF WHICH CELLULAR PROTEINS ARE ASSOCIATED WITH THE VIRUS IS A PREREQISITE TO MAKING A GODDAMN TEST KIT, WHETHER OR NOT IT IS PROTEIN OR NUCLEIC ACID BASED, AND THEN USING IT TO RISK THE LIVES OF MILLIONS OF PEOPLE WHO WILL BE FORCED TO TAKE DANGEROUS CHEMOTHERAPIES BASED ON A p24 test from the likes of this junk science.
Cheers,
andy
andy, you're a laugh a minute! please don't ever stop posting!!
Dale/adele,
Dr. Maniotis is your scientific elder, bow your head to him and learn something. Hes not bought off by the drug co's like Moore/Wainberg/Levy inc.
Dr. Maniotis, I was just wondering since you are in contact with many professors at the University if many feel the same way you do and are too afraid to speak out, or have most of them sipped the Wainberg kool aid and bought into all this?
Thanks keep up the good fight, most everyone who I talk to who learns about the "dissidents" views, recent college grads like myself, agrees with most of it, its just
a matter of getting the info out.
Dr. Maniotis is your scientific elder, bow your head to him and learn something.
cooler, you're a pretty funny guy as well. But you're right. Maybe I could learn something. I already know how to cut and paste of course, but should I some day decide to throw away years of scientific training and practice, Andy could no doubt teach me how to misread and misrepresent the scientific literature - although I doubt I could ever be as skilled at irrelevant bloviation as he has demonstrated himself to be.
Animal models for AIDS:
Miller RJ, Cairns JS, Bridges S, Sarver N.
Human immunodeficiency virus and AIDS: insights from animal lentiviruses.
J Virol. 2000 Aug;74(16):7187-95. Review. No abstract available.
PMID: 10906172
Hey Black Falcon:
You said:
Two claims from Maniotis' essay have been examined in detail (Laurent-Crawford and Barre-Sinoussi), and both are based on fabricated quotes.
That means that they are not just "mistaken"--they are fraudulent.
In one case Maniotis' defends his lie by explaining that he has told it so "many time before" that to him it sounds more true than the truth. In the second case, he has offered no explanation.
Two out of two claims fraudulent, yet somehow you assume all of the remaining claims are valid.
Let me give you a clue. Before buying a used car from Maniotis, have it inspected by a competent and independent mechanic.
Franklin, please don't confuse AIDS denial with science. The AIDS denial movement is political, not scientific, and in politics a lie repeated often enough is as good as the truth.
It does not really matter if HIV exists or causes AIDS as long as you can convince people such as the president of South Africa that it does not. Once enough people become convinced, you have won. In science, unlike politics, what the general public believes does not matter. The fact that people used to believe that the Earth was flat, and now most believe that the Earth is roughly spherical in topology, did not cause the sun to stop rising in the east each day.
In the USA, the AIDS denialist political movement has very little support, and it is unlikely to gain much support. More USA citizens believe they can get rich by giving Nigerian billionaire widows their bank account information, than believe that HIV has not been isolated.
The important points for the denialists though, are not convincing Americans, few of whom are at risk of infection. The important point is to convince the leaders of South Africa, Nigeria, and other nations to suspend or delay taking actions to fight AIDS, polio, and other infectious diseases in their countries. Do a GOOGLE search for [polio vaccine Nigeria] to find out how successful Andrew Maniotis and his coworkers have been in their efforts. Or use the http://tools.google.com/gapminder/ GapMinder tool to plot life expectancy vs per capita income to see how events have played out in South Africa from 1970 to 2005.
It is you people that are responsible for some hideous crimes. Monster doses of AZT in the 80's w/o informing patients that they were being put under long term chemotherapy
Ho's lie of hit hard hit early
100x the safe limit of mercury in vaccines in the 90's w/o even telling patients
Vioxx, selenemite
As cooler says, LOL. Andy's exposed what ten times now for fabricating quotes lying about sources at the best not understanding basic science. Instead of defending himself anymore which is I gues impossible he starts in with the aneuploidy. And then switches somehow to epigenetics to toot his own horn.
Has anybody on aetiology said aneuploidy does nothing in cancer? Or epigenetics? I just don't remember it. The problems people have with Duesberg is, he doesn't say aneuploidy has a rolle in cancer, he says aneuploidy is THE ONLY THING in cancer. And that's complete crap. Just like its crap to say Duesberg is the father of aneuploidy and cancer when hundreds or thousands of people worked on it before him.
Just like Andrew is the father of epigenetics. My ass. I was working with chromatin before Andrew even heard of AluI.
What a blowhard our little "scientific elder" is! But a very amusing one. So I agree with Dale.
?
The demographics have been changing since 1985. Nevertheless, the incidence of HIV infection is much higher in these risk groups.
People at "low risk" do get infected with HIV but at a lower rate than those who have high risk behaviour.
Firstly, most of the rejected blood units are rejected for reasons other than HIV infection. Nevertheless, as the very papers we have been discussing demonstrate, even blood donors that are not excluded by the questionnaire still turn up HIV positive but at a lower rate than people that fit in the high risk categories.
Andrew,
I think you may have made a breakthrough. Your rambling post on the DAIDS Manual provided the most clearly true statement on HIV/AIDS that I have ever seen from you:
I have read and re-read your post several times and carefully gone through the relevant protocols you cite from the DAIDS Manual, and I can assure you that the explanation you offer, namely, that you "really don't understand what is going on" is absolutely, 100% on target.
As already explained by Dale, the assay requires non-infected cells. It is the ability of the patient specimen to induce a productive infection of the normal cells that forms the basis of the assay. The stipulation that the normal cells should not be older than 3 days post-stimulation is a quality control mechanism to make sure that they are still able to support a productive infection and thereby avoid false negative results that might be obtained using older cells. This is very clearly explained in the DAIDS Manual, as well as in the papers cited in the bibliography included in the DAIDS Manual. The fact that the use of non-infected cells is "irrational to your way of thinking" simply illustrates that you have no clue as to how the assay works and proves that (as you put it) you "really don't understand what is going on."
In the interest of full disclosure to your future readers, I would suggest that you append that disclaimer on any future writing you do with respect to HIV/AIDS. A good place to start might be the corrected version of your "ABC's" essay--you know, with the corrections in which you remove all of the bogus quotes. (You can add your allusion to the DAIDS manual to your list of false claims in need of correction.) The new title should look something like this:
The ABC's of AIDS Denialism (Unless I Really Don't Understand What's Going On)
By: Andrew Maniotis, Ph.D.
Testing for censorship
thanks. by Brooklyn