
Over the last two or three weeks, you might have noticed a disturbance in the alternative medicine force. Unlike disturbances in the Force in Star Wars movies (which usually result from horrors like the obliteration of millions of lives on Alderaan), this was a joyous, celebratory disturbance in the mystical nonexistent energy fields in which promoters of alternative medicine cancer cures and haters of chemotherapy and "conventional" cancer treatment (the two almost always go together) thought that a major study in a reputable journal had put yet another "final nail in the coffin of chemotherapy." Or at least they could spin the study as an indication that chemotherapy is nothing more than an expensive toxic brew foisted on an unsuspecting public by the nefarious shadowy forces of Big Pharma in order to extract maximal resources from third party payers, which, to them, is almost as good. Of course, they do this with any study that suggests chemotherapy isn't as effective as people would like, but this study seemed on the surface like powerful ammunition. It's not. It's actually an interesting preclinical study showing a mechanism by which chemotherapy given before surgery (neoadjuvant chemotherapy) might promote the spread of some cancers. Whether the findings are clinically important remains to be seen.
"Alternative cancer cure" advocates and salesmen rejoice
Although it's an interesting study delivering somewhat of a cautionary note, The study being gloated over is far less of a "black eye" to chemotherapy (as Jeffrey Jaxen put it over at that repository of science misinterpreted to promote alternative or "natural" medicine, Sayer Ji's GreenMedInfo), than advertised. (Besides, Ji likes me. He really, really likes me.) Meanwhile, Chris Wark of "Chris Beat Cancer" (hint: surgery, not the quackery he pursued, took care of his colon cancer) practically exults that "chemo may spread breast cancer and trigger more aggressive tumors." Of course, the real gloating comes from—who else?—Mike Adams, who proclaims the study a "Medical BOMBSHELL" showing that chemotherapy has been found to spread cancer. He also can't help but throw in the lies he's been peddling about me as well.
Yawn. I guess I can expect attacks like this inserted into pretty much any rant against chemotherapy that Adams writes from now on. It's my badge of honor. Oh, well. Word to Mikey: I used to be upset by your smear campaign against me—about a year ago. These days, however, I'm laughing at you, not with you, because your lies are so transparently over the top that no one but your hardcore followers would even have a chance of believing them. I was never a "colleague" of Dr. Fata, who never worked at my cancer center, and that "nipple ripper" name came from Patrick "Tim" Bolen, a man who used to be cancer quack Hulda Clark's most vigorous defender. I also note that it was Adams himself who claimed to have reported me to the FBI (something conveniently not mentioned). That was well over a year ago. Neither I nor anyone I know has been contacted by the FBI or my state attorney general (where Adams also claims to have filed a complaint). I suspect his "criminal complaints," if they were ever filed at all, ended up in the "crank file," where they belong.
Let's get back to what less insane-sounding (but equally mistaken) alternative cancer cure advocates are saying, after which then I'll delve into the study itself and show you why, although it is a reason for some concern, it's not evidence that chemotherapy doesn't work, and, in fact, if validated by further studies, points the way to overcoming what might be a significant problem in cancer chemotherapy. In discussing this study, Jaxen, for instance, lists all the usual suspects of studies trotted out by the anti-chemotherapy brigade every time they feel a rant coming on. For example, he invokes what I like to call the "2% gambit," citing, as all who use this gambit do, a single Australian study from around 16 years ago that left out a lot of chemotherapy-sensitive tumors and willfully confused adjuvant chemotherapy with chemotherapy delivered as primary treatment for curative intent. Basically, he sees the study as "more evidence" of this:
By now, many are beginning to understand that one of the problems with chemotherapy is that it doesn’t address the underlying cause(s) of cancer. Chemotherapy originated from an idea and consciousness that was far from idealistic. The whole generation of chemotherapeutic drugs that are being used today, and there are over one hundred of them, developed from poisonous nerve gas created for warfare. As reported in 2012 by Green Med Info, cancer is the second leading cause of death in the developed world, and yet much of the medical and research communities are still in the dark ages when it comes to treating and understanding it. However, in the age of information, great strides are being made by doctors and researchers who are going against the grain of the failed convention ‘wisdom’ in cancer treatment. In addition, individuals are beginning to take responsibility by educating themselves.
Of course, for all their claims of "addressing the underlying cause" of cancer, alternative medicine cancer cure mavens always fail to show how their favored nostrums do any better on that score, much less that they are actually more effective than conventional treatments—or even that they're effective at all.
Chris Wark chimes in with the same propaganda:
As I’ve said many times, chemotherapy is often only a short-term solution to a long-term problem.
The new study presents evidence that chemotherapy can switch on a repair mechanism in the body which ultimately allows tumours to grow back stronger. It also increases the number of ‘doorways’ on blood vessels which allow cancer to spread throughout the body.
At least Wark admits that chemotherapy can sometimes be at least a "short term solution" to cancer. Again, nothing Wark discusses shows how his preferred methods do anything to "address the underlying cause" of the long term problem of cancer. We know that diet and certain environmental exposures can modulate cancer risk for certain cancers, but once the cancer is already established it's too late for that.
So now that we've seen ideology in action, let's look at science in action.
How chemotherapy is used to treat cancer
Before I get to the study, in order to help readers not familiar with how chemotherapy is used to treat cancer, I feel obligated to provide a brief primer. There are four main ways that chemotherapy is used to treat cancer:
Curative: Chemotherapy can be the primary (and sometimes only) treatment for cancer. This is common in hematological malignancies, like leukemia and lymphomas, where it's usually some combination of chemotherapy ± radiation therapy that is curative. Surgery is rarely indicated. The intent here is to use chemotherapy to eliminate cancer from the body.
Adjuvant chemotherapy: After definitive surgical treatment of the primary cancer, chemotherapy is administered to decrease the chance of recurrence. This is a very common use of chemotherapy, particularly in breast cancer and colorectal cancer. Indeed, the use of adjuvant chemotherapy for breast cancer since the 1980s, among other factors, has contributed to a decline in breast cancer mortality of around 30% since 1990.
Neoadjuvant chemotherapy: Neoadjuvant chemotherapy is administered before surgery. In general, there are two main reasons to administer neoadjuvant chemotherapy: (1) to shrink a tumor to make a non-operable tumor (e.g., one stuck to major structures) operable for cure; and (2) to make organ-sparing surgery possible. This latter use is common in breast cancer in order to shrink a tumor so that a mastectomy is not required to remove it and breast-conserving surgery is possible. Moreover, in breast cancer, it is known from numerous studies that neoadjuvant chemotherapy results in equivalent results as adjuvant chemotherapy. Overall survival and disease-free survival and time to locoreginal recurrence are the same, whether chemotherapy is administered before or after surgery. The same idea is used in the surgical treatment of low rectal cancer requiring an abdominoperineal resection (APR) to remove. An APR involves removing the anal sphincter and leaving the patient with a permanent colostomy. With neoadjuvant chemotherapy, it is often possible to shrink the tumor enough to make sphincter-sparing surgery possible, something very desirable to patients, the vast majority of whom understandably recoil at the idea of requiring a permanent colostomy.
Palliative chemotherapy: In stage IV disease, chemotherapy is often used to palliate symptoms from growing tumors and can prolong life, although not result in long term survival. This is also a common use of chemotherapy.
The study that the likes of Mike Adams and Chris Wark are crowing over examines neoadjuvant chemotherapy. That's an important point. It does not apply to other uses of chemotherapy. Think of it this way. Adjuvant chemotherapy is quite different from neoadjuvant chemotherapy in at least one way. The primary tumor is not present when adjuvant chemotherapy is administered. All that's left are microscopic tumor deposits that could turn into metastases. Those are what adjuvant chemotherapy targets, because chemotherapy is much better at wiping out microscopic tumor deposits than macroscopic tumors. Contrast that to neoadjuvant chemotherapy, which targets both those same microscopic tumor deposits and also targets the main tumor, which is usually large. (Remember the reasons why neoadjuvant chemotherapy is administered.)
Comparatively speaking, there are many orders of magnitude more cancer cells in the neoadjuvant setting than in the adjuvant setting. If spread of tumor due to neoadjuvant chemotherapy were a major factor clinically, we'd expect survival using neoadjuvant chemotherapy before surgery to be worse than using it after surgery. That we don't observe worse outcomes with neoadjuvant therapy is a good reason to be at least a little skeptical of how clinically relevant the results of this study will turn out to be. Indeed, I've never ceased to be amazed that, in breast cancer and most cancers for which neoadjuvant chemotherapy is used, the survival benefit provided by chemotherapy (adjusted for tumor stage and other relevant characteristics, of course) is the same regardless of whether the chemotherapy is administered before or after surgery. Even better, neoadjuvant chemotherapy can give an indication of how "nasty" (i.e., resistant to chemotherapy) a tumor is, based on how much (or how little) it shrinks in response to chemotherapy. Moreover, pathologic complete response (that is, a response so dramatic that the tumor not only disappears clinically but the pathologist can't find any viable tumor cells in the resected specimen) is an excellent prognostic factor predicting favorable outcomes.
Keep these things in mind as I discuss the study.
Does neoadjuvant chemotherapy "spread" cancer?
So let's take a look at the study itself (Karagiannis et al, "Neoadjuvant chemotherapy induces breast cancer metastasis through a TMEM-mediated mechanism"), which was published in a Science journal, Science Translational Medicine by a group at the Albert Einstein College of Medicine. Reading the abstract, I quickly realized—surprise! surprise!—that the findings were considerably more nuanced and interesting than Adams, Wark, and Jaxen presented. I also quickly realized that the purpose of the study was to identify potential problems with how neoadjuvant works in order to find strategies to make it work better. Of course, doing research to make existing therapies better is complex, and the authors noted that increasing tumor cell dissemination could "diminish the clinical benefit" of neoadjuvant chemotherapy. Note the distinction. It is known—sorry, couldn't resist a Game of Thrones reference given that as I write this the season seven premiere is only a few hours away—from numerous studies that neoadjuvant chemotherapy produces a survival advantage for breast cancer patients in addition to the advantages it produces in making inoperable tumors operable or making it possible for women who would otherwise lose their breast to preserve it. Tumor cell dissemination as a result of chemotherapy reduces, not eliminates, that benefit, and it certainly does not "make cancer spread" in such a way that neoadjuvant chemotherapy is worse than no chemotherapy. Yet that's what the cancer quacks strongly imply.
So what is the mechanism being examined here? Previous work has demonstrated one mechanism by which breast cancer cells can gain access to blood vessels and spread. In this mechanism, breast cancer tumor cell spread occurs at microscopic structures dubbed tumor microenvironment of metastasis (TMEM). Each TMEM is composed of three cell types, all in direct physical contact with each other: a tumor cell making a protein that regulates a structural protein (actin) known as Mammalian-enabled (MENA), a perivascular macrophage (an immune cell near the blood vessel), and an endothelial cell (the cell type that lines blood vessels). Vascular permeability due to TMEM has been shown to be localized and mediated by vascular endothelial growth factor–A (VEGF-A) release from the TMEM-bound macrophages, which express the angiopoietin receptor TIE2. Now, I used to do a lot of work with VEGF-A back in the 1990s, when I studied tumor angiogenesis, the process by which tumors interact with their environment to stimulate the ingrowth of new blood vessels. Basically, the macrophages associated with TMEM secrete this factor, which increases vascular permeability, making "holes" through which tumor cells can gain entry to the blood vessel and spread via blood. However, only tumor cells expressing high levels of MENA can take advantage of this. (Note that there are different isoforms—variants—of Mena that are pro-invasion and anti-invasion; when we refer to MENA here, we're mostly referring to the MENAINV.) Tumors with a high TMEM “score” in animal models have a higher likelihood of metastasis compared to tumors with low TMEM scores.
The authors hypothesized that preoperative chemotherapy could increase the density and activity of TMEM sites in breast cancer, as well as an increase in invasion-promoting MENA isoforms, and thereby increase the number of tumor cells spreading. They based their hypothesis on the observation that one chemotherapy agent, paclitaxel (a.k.a. Taxol), induces an influx of macrophages into the primary tumor and that macrophages are required for TMEM assembly. The hypothesis was tested using a transgenic mammary tumor model in which mouse mammary tumor virus–polyoma middle T antigen was introduced to produce a mouse strain that spontaneously develops mammary tumors at a high rate, patient-derived xenografts (PDXs, which are tumors derived from patients that can grow in mice with defective immune systems), and pre- and post-neoadjuvant breast cancer tissue samples from human patients. There are also all sorts of pretty images from intravital imaging (IVI, which allows imaging of living animals at a cellular level) that a researcher needs if he wants to publish in a journal like Cell, Science, or Science Translational Medicine. I don't mean that so much as a knock on the authors given that the paper is actually good, but rather as a sarcastic aside at what it takes these days to be published in top-tier journals. Besides, several of the authors have an extensive background in imaging research; so I can't really fault them for using it. It is, after all, so much cooler to look at these complexes in living mice than to do what they had to do in humans and test fixed tissue from biopsies and surgical specimens.
The authors addressed their hypothesis using multiple tumor models, including the MMTV-PyMT mice, another mouse strain bearing tumors transplanted from the MMTV-PyMT mice, and two PDX models, (HT17 and HT33, for anyone who's interested). Animals were treated with various chemotherapeutics and compared to controls, with the tumors imaged, levels of various RNAs and proteins compared, and tumors assessed. Key findings were as follows:
- Paclitaxel at the dose used delayed tumor growth (as expected) but increased TMEM assembly by as much as three-fold.
- Paclitaxel increased the infiltration of perivascular macrophages in the primary breast cancer microenvironment.
- Paclitaxel induced TMEM-dependent vascular permeability in breast tumors.
- Paclitaxel increased metastatic dissemination of breast tumors (roughly a two-fold difference, although the result wasn't statistically significant for one tumor model—Figure 3I). This was confirmed by examining the lungs of the mice, where investigators found an increase in both microscopic metastases in the paclitaxel-treated mice and single-cell metastases (two-fold increase).
- Paclitaxel promotes the expression of invasive isoforms of Mena in breast tumors, and dissemination required Mena.
- Levels of circulating tumor cells in the bloodstream increased in response to chemotherapy.
- Treating mice with doxorubicin and cyclophosphamide (two other drugs commonly used in standard-of-care breast cancer treatment) produced similar changes in the primary tumors and their surrounding microenvironment.
Finally, when the investigators tested human breast cancer tissue before and after neoadjuvant chemotherapy with paclitaxel followed by combined doxorubicin/cyclophosphamide, they found this:
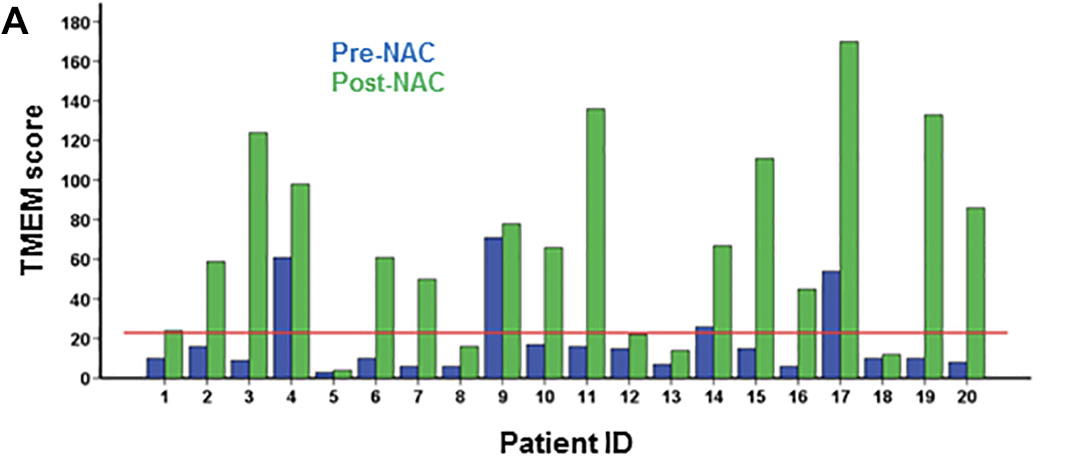
Areas staining positive for MENA also increased. Pretty striking, I'll agree. However, remember what I said above. Neoadjuvant chemotherapy is still quite effective.
More importantly, consider this final result. In the same mouse models, blocking the TIE2 receptor with rebastinib decreased the number of perivascular macrophages and blocked the increase in circulating tumor cells to the level of controls without affecting TMEM assembly. This means that TIE2 inhibition blocks the function of TMEM sites but not their assembly. Fortunately, in these mouse models, that was enough. More importantly, it also suggests a strategy for making neoadjuvant chemotherapy work better in patients, as illustrated here:
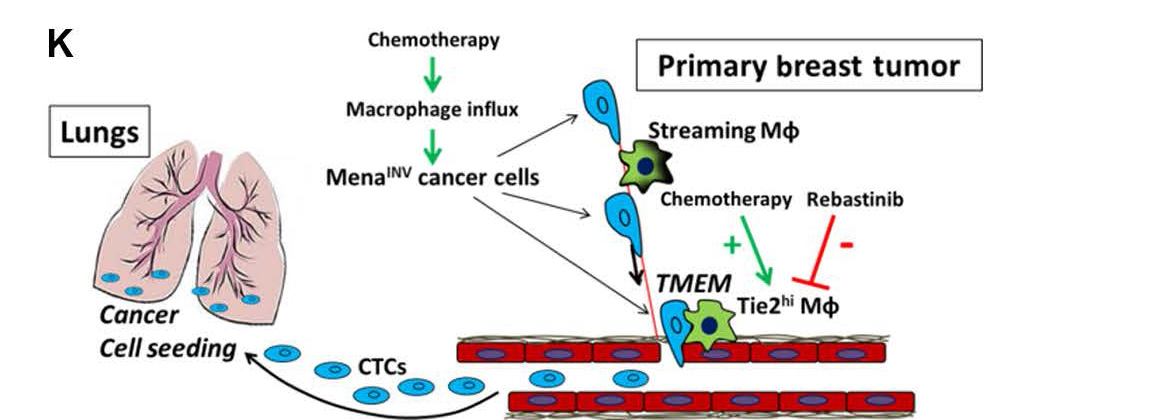 How cancer spreads via the bloodstream.
How cancer spreads via the bloodstream.
Note that there are multiple points that can be attacked to overcome the stimulation of more invasiveness by chemotherapy.
Putting it all together
If there's one thing that distinguishes science-based medicine (SBM) from the sort of medicine advocated by those promoting alternative cancer cures, it's that SBM is always trying to make things better. When it is observed that, for instance, neoadjuvant chemotherapy might not be having as strong an effect on tumors as it could, scientists look for the reason why. If that reason why happens to be that some forms of chemotherapy might increase the ability of cells from the primary tumor to spread, decreasing the benefit of neoadjuvant chemotherapy, they look for the molecular and cellular mechanisms responsible for that problem and then try to find ways to exploit those mechanisms to overcome the problem. That's exactly what Karagiannis et al did. So when quack-loving entrepreneurs like Mike Adams, Chris Wark, and Jeffrey Jaxen tell you this study "proves" that chemotherapy does more harm than good, they're either ignorant or intentionally misrepresenting the results, because the study doesn't show that at all.
It's not just the quacks, though. Articles in mainstream news sources reported this study with headlines like "Chemotherapy could cause cancer to SPREAD and grow back even more aggressive, new study claims." OK, that's The Daily Mail, which is to science as The Weekly World News is to, well, news. But other stories had headlines like "Chemotherapy could spread cancer cells and lead to more advanced tumours, says study" and "Chemotherapy before breast cancer surgery might fuel metastasis." Far better is a headline like "Neoadjuvant Chemotherapy Treatment May Increase Risk Of Breast Cancer Spreading In Some Patients", which more accurately assesses the results of the study. In fairness, I know that editors, not reporters, determine headlines and most of the mainstream articles I mentioned did point out some of the caveats that I discussed, but the impression most people take away comes from the headline, and that impression was only marginally less scary than the headlines coming from Sayer Ji's and Mike Adams' websites.
More importantly, if you're a woman considering neoadjuvant chemotherapy to treat breast cancer, don't let the spin on this study frighten you out of it. The benefits of neoadjuvant chemotherapy include not only improved survival but the possibility of breast conserving surgery, and, as I mentioned before, there is no detectable difference in overall survival whether chemotherapy is administered before or after surgery.
As for the future, research like this could lead the way to better neoadjuvant chemotherapy. For example, a woman undergoing neoadjuvant chemotherapy might some day have biopsies done part way through the chemotherapy. If her tumor's TMEM score has increased markedly, then I could envision the addition of a TIE2 inhibitor or other inhibitor of TMEM function being added to her chemotherapy to block the increased level of circulating tumor cells and reverse whatever increased risk of metastasis that might be attributable to neoadjuvant chemotherapy in order to produce better outcomes. That's how SBM improves, in contrast to alternative medicine, in which no therapies are abandoned when demonstrated to be ineffective and/or dangerous and no therapies are ever improved upon.
"developed from poisonous nerve gas created for warfare"
Nice scare dogwhistling. Also a bit of a research failure isn't it? Relatives of Mustard Gas were (probably still are) used in chemotherapy - but Mustard Gas is not a nerve agent.
OK, so quite a bit of this is way over my head. But let me see if I understand what's going on here.
What we're really talking about with neoadjuvant chemotherapy is a side effect, yes? An unanticipated adverse reaction where the improvements (smaller tumor) come with a cost that can be adjusted for with other therapies.
Someone ought to tell Mikey, "and in other news, water is wet."
@Orac,
You are smarter than the above-average bear when it comes to convincing the masses that the biological mechanism-of-action is always the desired goal of science-based medicine.
"When you come to a fork in the road, take it." Yogi Berra
"Relatives of Mustard Gas were (probably still are) used in chemotherapy"
Spot on - L-phenylalanine mustard, AKA melphalan and a couple of trade names, is still useful in chemotherapy. Unlike many other chemotherapeutic drugs, it can be given in tablet form as well as by intravenous infusion.
Daily Mail
"We are no longer accepting comments on this article."
Bah, too late :'(
But not even "mustard gas" is actually a gas. It has a boiling point of 423 °F.
Nor does not come from mustard; it smells like mustard (allyl isothiocyanate). It is totally synthetic.
And the "nitrogen mustards"—named by analogy to "mustard gas" by substituting N for S—don't even smell like mustard at all. The most structurally analogous N-mustard (chlormethine) has a "faint odor of herring". It should be called "herring gas".
https://pubchem.ncbi.nlm.nih.gov/compound/mechlorethamine#section=Exper…
And it has a boiling point of 189° F, making it also not a gas. ("herring liquid"?)
Phenylalanine "mustard" is even further removed from chlormethine (which isn't even a gas and doesn't even smell like mustard.)
It becomes clear that the term "mustard gas" is a highly-enriched, nuclear-grade misnomer. What all of these chemicals have in common is their ability to alkylate tissues through an "epoxide"-type intermediate* as the molecule loses Cl⁻ in water. They can do this twice (once on each end of the molecule) and can crosslink proteins and DNA similar to malondialdehyde (watch out lysine!).
It crosslinks DNA, as shown by changes in viscosity and increased dehybridization temperature.
Inter-strand Crosslinking of DNA by Nitrogen Mustard (Kohn 1966)
Personally, I think we should all call them "epoxide-like alykylation agents" from now on. This "mustard gas" name should be reserved for bischloroethyl sulfide only.
*MJD is going to take this thought straight to the Glue Department at 3M. (I predict we will see "Mustard Glue™" on the shelves in ~7 years.)
You mean* "mustard" isn't already one of the three "M"s?
* ...mister...
aairfccha: "Nice scare dogwhistling. Also a bit of a research failure isn’t it?"
What else should you expect from Green Med Info?
That duck will never fly, even with latex wings.
but Mustard Gas is not a nerve agent.
Ah well. "Poisonous nerve gas created for warfare” -- as opposed to all those poisonous nerve gasses created for civilian applications -- is just a string of Worship Words for GreenMedInfo readership.
Abbey Road isn't my favourite Beatles album (Rubber Soul is), but I am quite attached to that song (it's almost as catchy as Maxwell's Silver Hammer).
You could almost say that it has bonded with me.
I think it was Paul, since it adheres very well to McCartney's prior songs. [It couldn't have been Ringo.]
This last Sunday on CBS "Sunday Morning" the whole episode was focused on cancer. I cringed at the start because, in reviewing the history of cancer, it was noted how in the mid-1900's doctors started using "toxic" chemicals to treat cancer. At least I didn't hear "toxins".
Ugh, your blog posts read like trash celibrity stories, throwing the "quack" word around and making tacky insinuations, I cannot stomach it. Can't you just keep it to the point and factual? If your facts stand, they should do the job of exposing quacks just fine (or even: much better).
Here is a suggestion, Maarten: don't read it.
Chris, I will avoid reading it, but at the same time I'm interested in finding a website that critiques the alties in a constructive manner. I don't know if you have some good suggestions, but if you do, I would appreciate it.
"Alties"? That sure sounds derogatory. That doesn't sound very constructive at all to me! After all "alties" is a term I used to use but rarely do any more because it makes fun of the quacks' marks. Perhaps you should be a little less self-righteous.
Maarten: if you think it would work, why don't YOU start one? Instead of b****ing at Orac?
It's OK. He's just a typical self-righteous guy who's more concerned with tone than with the actual harm quacks do. Having personally seen the harms done by quacks on my own practice and heard countless stories over the years of the harm done by cancer quacks, not to mention having had quacks like this try to get me fired from my job, I make no apologies for taking a—shall we say?—insolent tone when refuting them. I really don't care if people like Maarten clutch their pearls when they encounter it.
Also, Maarten is clearly a newbie here. I use a variety of levels of insolence depending on the topic (and my mood). This blog would become mighty boring (both to readers reading it and me writing it) if I were to start writing the way Maarten seems to prefer. I decline.
Maarten: I like Panacea's suggestion @#17. I believe I can provide some 'constructive' advice.
.
First, we need a respectful term. May I suggest 'Medical Charlatans'?
.
Next we need to agree upon some basic facts.
1. Most MC's are spreading their 'knowledge' in pursuit of fame and/or fortune.
2. In general, their 'knowledge' can, and has, harmed people. This harm includes death as an identifiable risk
3. We can conclude from #1 and #2 that they are, in general, potential killers and their victims include people we know.*
.
Sounds like you've got a killer blog on your hands! There's no telling how many clicks you'd get with a blog named
LET'S ALL BE NICE TO THE PEOPLE TRYING TO KILL US
.
* This isn't abstract knowledge. My wife died of cancer last year, and I got used to telling people that I'd check with the oncologist and nephrologist about their suggested 'treatments.' If they inquired again I'd tell them that the 'treatment' hadn't been tested with Multiple Myeloma patients who had kidney failure. Most people dropped it, but those who pushed the issue were sent to check and see if the Medical Charlantry Miranda warning (formerly known as the Quack Miranda warning,) was invoked. That shut them up..
Maarten: "I don’t know if you have some good suggestions, but if you do, I would appreciate it."
Why should I do that for you? Do you own homework. There are plenty of good doctors/scientist blogs that discuss these subjects. Many have been linked to from this blog. Though if you don't like the tone of this blog, you are going to hate SciBabe.
@ Opus:
re:
LET'S ALL BE NICE TO THE PEOPLE TRYING TO KILL US
You're right.
I spend a great deal of time listening to and reading material that endangers health and simultaneously is extremely vicious 'reporting' on SBM and actual health care providers.
I don't think that we should be nice at all.
We should expose charlatans, quacks and cranks as a service to those who are potentially their victims.
Since they eternally harp upon how much money pharma and SBM make, we can easily show that they are not exactly living on Poverty Row
- plus, unlike real meds, BS meds cost little. If you manufacture vitamins for a small sum and then, market them as cure alls at a high price, that's easy to illustrate.
And it's all over the met.
@Orac#16 I think that if I would be searching for an alternative cancer cure, then I would not mind being called an "altie", but you may be right that this word could be derogatory. Still, it's much better than "quack" in my opinion.
Also, I must say that this blog post is much better than the "Pharma hit squads one", which I read first and I found really distasteful (so when this post started with a dubious reference to The Force, I stopped reading because I had enough, where I should have continued to read).
And I know I am self-righteous, but my impression so far is that you are too.
I have a question about your statement, maybe you would be willing to explain:
"We know that diet and certain environmental exposures can modulate cancer risk for certain cancers, but once the cancer is already established it’s too late for that."
How do you know that its not possible through diet to give the body a significantly increased change to beat an established cancer? Saying it's not possible (or that there is no reason to assume that it could be possible) seems quite a claim.
Maarten: "How do you know that its not possible through diet to give the body a significantly increased change to beat an established cancer? Saying it’s not possible (or that there is no reason to assume that it could be possible) seems quite a claim."
How would that work? What specific biochemical processes coming through the gastrointestinal track would affect the abnormal growth of cancer cells?
Very good question Chris - and one that I ask often.
If a person makes that claim that doing "something" to the body will help fight Cancer, I ask - okay, so exactly by what biological mechanism would this "something" help?
It is something that keeps coming up. During one discussion half a dozen years ago I even downloaded a book by a (literally) die-hard fan of food curing cancer, and read it. I found it lacking:
http://scienceblogs.com/insolence/2011/08/02/rip-david-servan-schreiber…
If Maarten could go over there and find the missing cites that I kept asking for, that would be very nice.
Chris, it's interesting that you use the word "lacking", and not "nonsense" or "hogwash". I will try to make the list of cites you asked for and post it here hopefully soon. I can already say that it's strange to ask for an *exact* biological mechanism just to support my claim that it could be possible that a change in diet significantly increases the bodies ability to heal itself from cancer (if someone is eating poorly and has - for example - chronic headaches that have no direct explanation, wouldn't you advise them to start eating healthier because *maybe* there is a relation between their diet and their headaches?)
Postulating a biological mechanism gives a head start on deciding which (of the hundreds) of kinds of cancer you could address with your postulated change of diet. It also gives a clue as to what stage of that cancer it could help with. It would also help predict interactions (and interferences with standard-of-care therapies that will be used with your diet changes.
A claim that it could be possible is useful for only two purposes: (a) preparing for planning of clinical testing or (b) inventing a pseudo-science claim to support (e. g.) advertising for yet another Cancer Cure!!!!! book. "Could be possible" isn't useful by itself in science or in real life; it's plenty for a woo-grifter, though.
Maarten -
As an example: You can dramatically reduce your risk of getting lung cancer by not smoking. However, once you have lung cancer, stopping smoking will not cause it to regress.
Or as an analogy.. I can reduce the risk of fire in my house by insisting on only the bast and safest electrical appliances. However, if my house is on fire, upgrading all my electrics will do nothing to stop it.
It's possible that there is some change in diet that can affect the course of cancer, but it would be a horrendously difficult study to do; you'd be looking at a minor effect (probably) and have to persuade a great many cancer patients to change their diets and stick with the new diet for a considerable period of time. Hard work.
Any food that helps treat an already established cancer will probably also have these side effects.
https://www.cancer.org/treatment/treatments-and-side-effects/treatment-…
Any effect a healthy diet would have on cancer would probably be to help the cancer grow. It would give the tumor cells the resources they need for replication and to build new circulatory networks to keep those resources flowing.
The converse doesn't mean it would hurt the cancer, since tumor cells are very good at appropriating resources for their own growth, which is why cancer patients lose so much weight.
Honestly all diet will do for you is let the cancer kill you more slowly.
Chris, to answer your question: diet may impact cancer growth through its relation to the IGF-1 levels in the body. The reasons to consider this possibility are:
- IGF-1 is directly involved in (tumor and normal) cell growth
- Congenital IGF-1 deficiency is associated with dramatically lower cancer rates
- vegans have significantly lower IGF-1 levels and higher IGF-1 binding capacity (suggesting that the IGF-1 level can be directly influenced by diet)
References to scientific papers are given in these short videos from which I learned these findings:
- https://nutritionfacts.org/video/how-plant-based-to-lower-igf-1/
https://nutritionfacts.org/video/cancer-proofing-mutation/
- https://nutritionfacts.org/video/igf-1-as-one-stop-cancer-shop/
Based on this information, I would not exclude the possibility that adopting a vegan diet might significantly improve the bodies ability to fight cancer.
Videos? Anyway, as I've mentioned before, my best friend, a 20-year vegan, died of metastatic colorectal cancer at age 40 and never even got to see his second child. This brand of idiocy pisses me right the f*ck off.
ps I just learned that the ketogenic diet is another example of how diet *might* play a significant role in fighting cancer. Perhaps a ketogenic vegan diet would combine the benefits of both?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3826507/
Maarten: maybe you shouldn't exclude it but you certainly shouldn't include it.
This website is a prime example of the kind of thing I teach nursing students to avoid when citing sources, or educating patients. The website has an agenda, and that agenda is to sell products, specifically his books and podcasts. Dr. Gerger even has the gall to promote his site as a non profit 501(c)(3). Bascially, he's asking to be paid to promote an unproven point of view as science.
Panacea: if what he says is unbalanced, then which results and papers should he also have mentioned to present a balanced point of view regarding the relation between cancer and diet?
How about this one for starters?
https://sciencebasedmedicine.org/the-gonzalez-trial-for-pancreatic-canc…
Or PubMed links to studies that show a real benefit to nutrition in treating cancer.
As my phone won't display that PMC link, I must simply say that I can't wait to find out what the typical menu would look like on a "ketogenic began diet."
^ Freaking autocorrect: vegan, not "began."
"I would not exclude the possibility that adopting a vegan diet might significantly improve the bodies ability to fight cancer."
Remember to include the reality that adopting a vegan diet has never been shown to improve outcomes for cancer patients. Of course, you can speculate to your heart's content, connecting as many vague and disparate dots as you like.
squirrelelite, the research in that link doesn't involve a vegan diet. Vegetarians and meat eaters have comparable levels of IGF-1, as shown in the graph in the video that I mentioned (https://nutritionfacts.org/video/how-plant-based-to-lower-igf-1/)
Also, how would giving *more* evidence on the benefits of the vegan diet correct the supposed inbalance in his view? Isn't this balancing supposed to happen by giving evidence to the contrary?
But in any case, he mentions nutrition research regularly, such as in this video: https://nutritionfacts.org/video/best-supplements-for-prostate-cancer/
@Narad, I'm very sorry about your friend. I strongly oppose any claim or suggestion that vegans will never get cancer. The videos I posted contain clear references to scientific publications (the title and authors can be easily read off the screen).
Video pimp.
Maarten,
The "just look at the video" method of proof offered by your favorite website, and its selective reporting & poor objectivity, has been addressed by Harriett Hall.
Take a look at her critique of Greger's vegan claims.
https://sciencebasedmedicine.org/death-as-a-foodborne-illness-curable-b…
Elliot, how is "just look at the video" a method of proof? Why is a list of publications written in ascii characters worth more than the same list written as pixels in a series of video frames? If you really care, then I am willing to translate from pixels to ascii, but it seems like a silly exercise to me.
I thank you for the link to the critique of dr Gregors presentation, I will read it with interest and post back here later.
As my great grandfather, an editor at the Washington Post, said: never believe it until you read it in the cold light of print.
What that means is that speech and the spoken word (and video also) use tricks of rhetoric to specifically and deliberately to induce emotions, to cloud rational thought, to baffle and beguile. It forces the listener to move at the speaker's pace, not their own.
If you send me a video I know you've got something to hide.
rs, I object to the word pimp (especially because of connotation with sexual exploitation, yuck!)
Never use the word "zucchini" and "prostate" in the same sentence...
You might give Maarten the wrong idea.
Oooh, look it is videos! Woot, the type of "evidence" one resorts to when they have no clue how science works. And he even keeps posting to Greger's site even after being told not to! Seriously, Greger is not a reliable source of information:
https://sciencebasedmedicine.org/death-as-a-foodborne-illness-curable-b…
I only want to see PubMed indexed studies that prove that something passing through the gastrointestinal track causes the abnormal cancer cells to stop reproducing in vivo. So no petri dish studies!
Rats, I skimmed to fast and repeated Elliot's link.
"Why is a list of publications written in ascii characters worth more than the same list written as pixels in a series of video frames?"
Because they are usually peer reviewed for some semblance of accuracy and include references. Of course, instead of making us waste our time watching silly videos, then you watch them and transcribe the PubMed indexed studies that are mentioned. Come back and list those studies. Posting their identification numbers (PMID) is sufficient.
JustaTech, all claims in the video are backed by references (giving the titles and authors of the corresponding papers). I thought that was good enough. If instead of the video, I would give you the list of references cited in the video, without any narrative about why the information in these papers suggests a significant relation between diet and cancer, would you go through them and find out for yourself if such a relation exists?
Also, is a scripted presentation that different from a written blog post? I think it's not. Just as you can critique anything written in a blog post, so you can critique anything said in a video (I assume we're able here to pause the video if necessary and think critically about anything that's claimed). I think it's helpful that people go to conferences, hear inspiring talks, and then ask themselves: is this really true? If nobody tried to create compelling narratives, I think science would progress more slowly.
Chris, the videos contain the references (lots of them). You can just read the titles and authors of the papers right off the screen. I even mentioned this to you in my previous message: "References to scientific papers are given in these short videos from which I learned these findings"
But since everyone is making such a big deal out of it, I will extract the titles of the papers from these videos, tomorrow.
Maarten, have you read any of the papers referenced in the videos you want us to look at? If so, you really only need to point out, say, the top 2 or 3 that most support the idea "that adopting a vegan diet might significantly improve the bodies ability to fight cancer".
If you haven't actually looked at the papers, well, I expect a Gish Gallop.
Why not today? Do you have a zucchini to carve?
Be sure to get the journal reference, including the issue date, while you're at it; although any standard reference will do, like PMID# or NIH link.
Sorry, Sara, I clicked on the wrong "Reply" button.
Maarten: "But since everyone is making such a big deal out of it, I will extract the titles of the papers from these videos, tomorrow."
Good. That will give us a basis to judge Greger's data. Be warned, he is not considered a reliable source of evidence.
You could make the argument that a vegan diet with reduce the chance of getting prostate cancer by lowering IGF-1. Cancers of the breast and prostate are known to responsive to three things: steroid hormones, IFG-1, and eicosanoids.
But a vegan diet could increase eicosanoid production through linoleic acid.
linoleic acid ⟹ arachidonic acid ⟹ eicosanoids
A litany of rat studies from the late 70s and early 80s will confirm than linoleic acid consumption is proportional both to spontaneous cancer incidence and tumor size in chemical carcinogen models.
Eicosanoids work mainly through the PPAR receptors (I know that's a redundant acronym but bear with me). These are nuclear receptors—which interact with DNA directly—that can influence the entire transcriptome, making linoleic acid (through eicosanoid production) on the same level of cellular control as retinoic acid and thyroxine.
Although a dairy-free diet (not necessarily vegan) is bound to lower serum levels of both IGF-1 and steroid hormones (prostate and breast growth factors), it could potentially raise the production of prostaglandins and other eicosanoids. Care must be taken with a vegan diet to limit linoleic acid.
Through this mechanism is how the anti-cancer effect of fish oil (ω−3) is usually explained (free radical explanations fail, since fish oil has a higher iodine value). Omega minus three fatty acids positively interfere with eicosanoid production, likely by acting as enzymatic competitive inhibitors (ligands).
A study from Chapel Hill in the 90s took fat biopsies of confirmed cases of prostate cancer and found enough elevated linoleic acid* levels to calculate risk ratios of about five.
*Care must be taken to distinguish ω−6 linoleic acid with α-linoleic acid (ω−3).
How's the job search going, Travis J. Schwochert?
^ Oh, wait:
That's a keeper.
I feel like a vegan ketogenic diet should be called "Kaleo."
“Kaleo.”
;-)
It turns out that the links I posted are supplied with a transcript and list of citations! Just visit the link, and click on "sources cited" in the footer. Looking forward to leaving the discussion about "video as a format" behind now and hearing your reactions on the content.
You're exposing your ignorance Narad. Did you think it was a hyphen like most people?
The only reason I spelled it out was because I didn't want to begin a sentence with a lowercase Greek letter, and "Ω−3" would probably just confuse you further. Besides, most editors would prefer seeing sentences that didn't start with things like numbers or abbreviations. Some style guides even recommend avoiding sentences which begin with acronyms (although this is rife in the literature.)
I'll give you a break since you are obviously foreign.
Maarten, I'm not going to waste my time watching self serving advertisements.
Either YOU, using appropriate citations, explain your point, or you don't.
If you don't then you're admitting it's all BS.
Panacea, if you are unwilling to read dr Gregers transcripts and list of citations, then fine, don't. I won't pretend that I can make the case for a vegan diet better than he can. Maybe someone else here is open minded enough to take a look.
FTFY.
"open minded enough"
I knew someone like that. His brains had to be mopped up. It didn't take long.
Maarten, then cut and paste the citations here. You are making the claims, therefore you need to provide the PubMed indexed studies of those claims. We are not going watch videos nor wade through transcripts.
Chris, here you go:
Papers cited in https://nutritionfacts.org/video/how-plant-based-to-lower-igf-1/:
Allen NE, Appleby PN, Davey GK, Key TJ. Hormones and diet: low insulin-like growth factor-I but normal bioavailable androgens in vegan men. Br J Cancer. 2000 Jul;83(1):95-7.
Ngo TH, Barnard RJ, Tymchuk CN, Cohen P, Aronson. Effect of diet and exercise on serum insulin, IGF-I, and IGFBP-1 levels and growth of LNCaP cells in vitro (United States). Cancer Causes Control. 2002 Dec;13(10):929-35.
Allen NE, Appleby PN, Davey GK, Kaaks R, Rinaldi S, Key TJ. The Associations of Diet with Serum Insulin-like Growth Factor I and Its Main Binding Proteins in 292 Women Meat-Eaters, Vegetarians, and Vegans. Cancer Epidemiol Biomarkers Prev. 2002 Nov;11(11):1441-8.
Ornish D, Weidner G, Fair WR, Marlin R, Pettengill EB, Raisin CJ, Dunn-Emke S, Crutchfield L, Jacobs FN, Barnard RJ, Aronson WJ, McCormac P, McKnight DJ, Fein JD, Dnistrian AM, Weinstein J, Ngo TH, Mendell NR, Carroll PR. Intensive lifestyle changes may affect the progression of prostate cancer. J Urol. 2005 Sep;174(3):1065-9; discussion 1069-70.
Papers cited in https://nutritionfacts.org/video/cancer-proofing-mutation/:
Guevara-Aguirre J, Balasubramanian P, Guevara-Aguirre M, Wei M, Madia F, Cheng CW, Hwang D, Martin-Montalvo A, Saavedra J, Ingles S, de Cabo R, Cohen P, Longo VD. Growth hormone receptor deficiency is associated with a major reduction in pro-aging signaling, cancer, and diabetes in humans. Sci Transl Med. 2011 Feb 16;3(70):70ra13.
Papers cited in https://nutritionfacts.org/video/igf-1-as-one-stop-cancer-shop/:
Yang SY, Miah A, Pabari A, Winslet M. Growth Factors and their receptors in cancer metastases. Front Biosci. 2011 Jan 1;16:531-8.
Zhang Y, Ma B, Fan Q. Mechanisms of breast cancer bone metastasis. Cancer Lett. 2010 Jun 1;292(1):1-7.
Kleinberg DL, Wood TL, Furth PA, Lee AV. Growth Hormone and Insulin-Like Growth Factor-I in the Transition from Normal Mammary Development to Preneoplastic Mammary Lesions. Endocr Rev. 2009 Feb;30(1):51-74.
Salvioli S, Capri M, Bucci L, Lanni C, Racchi M, Uberti D, Memo M, Mari D, Govoni S, Franceschi C. Why do centenarians escape or postpone cancer? The role of IGF-1, inflammation and p53. Cancer Immunol Immunother. 2009 Dec;58(12):1909-17.
Endogenous Hormones and Breast Cancer Collaborative Group, Key TJ, Appleby PN, Reeves GK, Roddam AW. Insulin-like growth factor 1 (IGF1), IGF binding protein 3 (IGFBP3), and breast cancer risk: pooled individual data analysis of 17 prospective studies. Lancet Oncol. 2010 Jun;11(6):530-42
Rowlands MA, Gunnell D, Harris R, Vatten LJ, Holly JM, Martin RM. Circulating insulin-like growth factor peptides and prostate cancer risk: a systematic review and meta-analysis. Int J Cancer. 2009 May 15;124(10):2416-29.
Gronek, Piotr ; Rychlewski, Tadeusz ; Słomski, Ryszard ; Stankiewicz, Krystyna ; Lehmann, Joanna. Insulin-like growth factor 1. Studies in Physical Culture and Tourism. 2005;12(1).
Piantanelli L. Cancer and aging: from the kinetics of biological parameters to the kinetics of cancer incidence and mortality. Ann N Y Acad Sci. 1988;521:99-109.
CDC Growth Charts. CDC. 2000.
Papers cited in https://nutritionfacts.org/video/best-supplements-for-prostate-cancer/:
Jacobs DR Jr, Tapsell LC. Food, not nutrients, is the fundamental unit in nutrition. Nutr Rev. 2007 Oct;65(10):439-50.
Thompson HJ, Heimendinger J, Diker A, O'Neill C, Haegele A, Meinecke B, Wolfe P, Sedlacek S, Zhu Z, Jiang W. Dietary botanical diversity affects the reduction of oxidative biomarkers in women due to high vegetable and fruit intake. J Nutr. 2006 Aug;136(8):2207-12.
Lansky EP. Beware of pomegranates bearing 40% ellagic Acid. J Med Food. 2006 Spring;9(1):119-22.
Bhupathiraju SN, Tucker KL. Greater variety in fruit and vegetable intake is associated with lower inflammation in Puerto Rican adults. Am J Clin Nutr. 2011 Jan;93(1):37-46.
Ye X, Bhupathiraju SN, Tucker KL. Variety in fruit and vegetable intake and cognitive function in middle-aged and older Puerto Rican adults. Br J Nutr. 2013 Feb 14;109(3):503-10.
Lansky EP, Jiang W, Mo H, Bravo L, Froom P, Yu W, Harris NM, Neeman I, Campbell MJ. Possible synergistic prostate cancer suppression by anatomically discrete pomegranate fractions. Invest New Drugs. 2005 Jan;23(1):11-20.
Freedland SJ, Carducci M, Kroeger N, Partin A, Rao JY, Jin Y, Kerkoutian S, Wu H, Li Y, Creel P, Mundy K, Gurganus R, Fedor H, King SA, Zhang Y, Heber D, Pantuck AJ. A double-blind, randomized, neoadjuvant study of the tissue effects of POMx pills in men with prostate cancer before radical prostatectomy. Cancer Prev Res (Phila). 2013 Oct;6(10):1120-7.
Chrubasik-Hausmann S, Vlachojannis C, Zimmermann B. Pomegranate juice and prostate cancer: importance of the characterisation of the active principle. Phytother Res. 2014 Nov;28(11):1676-8.
Thomas R, Williams M, Sharma H, Chaudry A, Bellamy P. A double-blind, placebo-controlled randomised trial evaluating the effect of a polyphenol-rich whole food supplement on PSA progression in men with prostate cancer--the U.K. NCRN Pomi-T study. Prostate Cancer Prostatic Dis. 2014 Jun;17(2):180-6.
Stenner-Liewen F, Liewen H, Cathomas R, Renner C, Petrausch U, Sulser T, Spanaus K, Seifert HH, Strebel RT, Knuth A, Samaras P, Müntener M. Daily Pomegranate Intake Has No Impact on PSA Levels in Patients with Advanced Prostate Cancer - Results of a Phase IIb Randomized Controlled Trial. J Cancer. 2013 Aug 29;4(7):597-605.
Because if you count from the carboxyl end, it's a plus sign, amirite? No, Fucklesworth, only you and some Wikipediot thinks that that's a minus sign, viz., that working backward of the last letter in the Greek alphabet is an arithmetic operation.
It's a wonder you can even breathe.
Great. Do it yourself. I, for one, simply don't bother with such* videos, whether presented by Orac or the commentariat. I read.
* Yes, I'll cop to the occasional musical interlude, but I don't expect anyone to look at those, either.
I can't believe that you people are doubting Maarten. Obviously, lower levels of IGF-1 and steroid hormones would be expected to lower the incidence of prostate cancer.
There are dozens of studies proving how androgens stimulate the prostate. It's even common to refer to some prostate cancers as either "androgen-refractory" or "androgen-resistant".
Milk contains 5α-androstenedione and 5α-pregnanedione, and the concentration of total androgens is significant.
And the rBHG used in modern dairy production has been shown to raise IGF-1 levels fourfold in the amounts commonly employed.
More likely he doesn't have the links because he's never typed them into a browser and read those pages either. Otherwise it'd be a trivial matter to pull them out of the browser's history by typing a few characters of the domain name.
Well, Maarten, I can already see a problem with one of the studies you listed as a citation from the videos you're pimping.
I decided to grab one of the articles at random, and pull it for review. The one I chose was:
Ornish D, Weidner G, Fair WR, Marlin R, Pettengill EB, Raisin CJ, Dunn-Emke S, Crutchfield L, Jacobs FN, Barnard RJ, Aronson WJ, McCormac P, McKnight DJ, Fein JD, Dnistrian AM, Weinstein J, Ngo TH, Mendell NR, Carroll PR. Intensive lifestyle changes may affect the progression of prostate cancer. J Urol. 2005 Sep;174(3):1065-9; discussion 1069-70.
So here's my issue with this article. It doesn't actually measure the progression of prostate cancer. It measures changes in PSA, which we know isn't the most reliable marker (it's why the USPSTF no longer recommends routine PSA screening). That's the problem with citing a source that's as old as this one (12 years old). Science can change quite rapidly in that kind of time frame.
The time frame of the study was too short; only one year. It included other lifestyle interventions besides diet which were not controlled for in determining what really affected the PSA. Was it the diet or the yoga? They also dismissed a similar study with negative results because the diets in that study were not "as low in fat" and did not include exercise or stress management.
If the rest of your citations are this bad, then I am very glad I did not watch these videos. That would have been time from my life I never would have gotten back.
Elliot, Chris, I read the critique by Hall, it was interesting. This is my opinion on her points:
CVD:
The author (Hall) critices Greger for quoting an article by Caldwell Esselstyn. Indeed Greger is quoting a conclusion from that paper in the conclusion of his own talk. However, he has not used that paper in his argumentation (he came to this conclusion through other means), so weaknesses in that paper cannot invalidate his argument.
Cancer:
Hall criticises Greger for the same quote from Esselstyn. For the reason already stated, her point is moot.
Inflammation:
Hall criticizes Greger for citing a study (Vogel RA1, Corretti MC, Plotnick GD) that does not use a control group. However, a criticism of a study does not necessary make a criticism of an argument (Greger draws on various studies, and is therefore not necessarily constrained by a limitation in one of those studies). To summarize Greger's full argument: eating meat causes an inflammation reaction that puts arteries in a crippled state (not "cripple" them as Hall misquotes, because that term suggests that they remain in the crippled state, which they don't). This crippled state is caused by endotoxins unique to meat, whose access to the arteries is faciliated by properties unique to animal fat.
If Greger's claim holds that the inflammation is caused by factors present in meat but not plants (and obviously, Hall is free to attack him on this point, but she didn't), then Greger's argument is not invalidated by the absence of a control group in the study by Vogel et al.
COPD:
Greger only makes one reference to COPD in his talk: "Thankfully, COPD can be prevented with the help of a plant-based diet, and even treated with plants if you want to check that out." So he encourages the audience to check it out for themselves, but does not try to make an argument for the benefit of a vegan diet on COPD. So it's beyond me why Hall suggests that Greger's argument "relies on a study that measured exhaled NO", as he is not making any argument! In fact, while he briefly mentions COPD, Greger shows a slide from a different paper called "Impact of dietary shift to higher-antioxidant foods in COPD: a randomised trial". If you want to guess about Greger's reason for believing that a plant-based diet can prevent COPD, that paper would have been a better candidate.
Alzheimers:
Hall misquotes Greger by asserting that he said: “We’ve known for 20 years that those who eat meat are 2-3 times as likely to become demented as vegetarians.” He actually used the words "appear between 2 to 3 times more likely". This result is based on a matched study. A different non-matched study found no statistically significant difference. So does the absence of a result in the unmatched study invalidate the claim that "that those who eat meat—red or white—appear between 2 to 3 times more likely to become demented, compared to vegetarians"? I would say it depends on how you interpret the word "appear".
Other claims:
Hall again critizes Greger for flaws in a cited paper, without attacking his full argument. She writes: 'He cites a study concluding “Our results suggest that a decrease in meat consumption may improve weight management.” Suggest, may, decrease. Not veganism.' Attacking the paper only works if the validity of the argumentation hinges on it.
Hall writes: "He compares raw meat to hand grenades, because of bacterial contamination. If you don’t handle them safely, it’s like pulling the pin. Are we selling hand grenades in grocery stores?". It escapes me why the vending place of these items would preclude a comparison, maybe someone can explain. Then she writes: "This is a ridiculous comparison, and it ignores the fact that plant-based foods can be a source of contamination too." I agree there, it's quite ridiculous (I even take this comparison as a kind of joke, not intended very seriously).
What do other studies show about the Benefits and Risks of veganism:
Hall writes: "This study showed mortality from ischemic heart disease was 26% lower in vegans and 34% lower in lacto-ovo-vegetarians (in other words, it’s better not to eliminate milk and eggs)." That's interesting, but I would like to know if the difference of 8 percent points between vegans and vegetarians is statistically significant. The paper itself says:
- The number of vegans was small (n = 753 subjects, 68 deaths), so the analyses in Table 7⇑ were repeated with the inclusion of data from the Health Food Shoppers Study, making the assumptions that all nonvegetarians were regular meat eaters and that vegetarians who reported that they did not consume dairy products were vegans. This increased the number of vegans to 1146, of whom 165 died before age 90 y. However, the numbers of deaths from individual cancers among vegans remained small (range: 3–8). The death rate ratios for the vegans compared with the regular meat eaters from the other causes of death were: for ischemic heart disease, 0.89 (95% CI: 0.65, 1.24; NS); for cerebrovascular disease, 0.51 (95% CI: 0.26, 1.00; NS); for other causes, 1.39 (95% CI: 1.12, 1.72; P < 0.01); and for all causes, 1.06 (95% CI: 0.81, 1.38). However, these death rate ratios should be interpreted with caution because of the uncertainty of the dietary classification of subjects in the Health Food Shoppers Study.
- Mortality from ischemic heart disease among the vegans was slightly higher than among the fish eaters and the vegetarians, but the number of vegans was small.
Hall writes: "Another study showed that the healthiest people in Europe, the inhabitants of Iceland, Switzerland, and Scandinavia, consume large amounts of animal foods." This paper does not study the plant-based diet, so I fail to see the point (if these people are healthier than vegans, then I would be very interested).
Hall writes: "This study found no significant differences in mortality between vegetarians and nonvegetarians.". This paper also not study the plant-based diet. What is does say about vegans is: "In this article, the vegans are included with the vegetarians because there were too few deaths among the vegans to report separately." For some unexplained reason the "death rates of participants are much lower than average for the United Kingdom. The standardized mortality ratio for all causes of death was 52%". So it seems the sample was biased towards healthy people.
"There are risks". Yes, all vegans should take a B-12 supplement.
Confounders:
Hall writes: "The elephant in the room is weight loss. Vegans weigh less than meat eaters, and many of the benefts claimed could be consequences of weight loss, particularly in diabetes. And they could be a consequence of eating more fruits and vegetables, rather than avoiding meat and milk.". I agree, let's find out!
She also writes: "The data he finds most convincing are from the 7th Day Adventist study." Why is that the data that he finds most convincing? Personally, I think he is more excited about the IGF-1 findings.
She writes: "Until we have confirmatory data from other studies in a general population, I don’t think it is wise to hang our hat on these decades-old Adventist studies.". I agree that we shouldn't, and I don't think we hang our hat on this study.
Can diabetes be cured?
Hall writes: "He says it can be cured by a plant-based diet, but the general consensus of medical experts is that diabetes can’t be “cured.”" The general consensus has changed in the past, often.
Other diet beliefs
Hall writes: "If the evidence were really so clear-cut in favor of veganism, we wouldn’t have all these differing approaches." Well, maybe people simply haven't heard the evidence. Many people don't even know what a vegan diet is.
What about the Eskimos?
"Blubber is a staple of the Inuit diet, and it contains large amounts of antioxidants. Atherosclerosis is practically unknown in Greenland. In Uummannaq, Greenland, a population of 3000 residents had no deaths due to CVD in the 1970s."
By all means, let's find out why the people eating blubber have much lower CVD than regular meat eaters. These foods are usually not included when comparing a plant-based diet to a standard diet. Maybe, instead of switching from regular meat to plants, some of us can switch to seal and whale.
Panacea, I'm sorry I made you loose time. You might be right, perhaps the drop in PSA was not indicating a change in the cancer growth, and if it did, maybe it was of some of the other lifestyle changes, not the vegan diet. I won't ask you any further to consider that maybe diet has something to do with it.
No, as a remarkably stupid choice versus, say, "Omega-3," like the rest of the known universe writes, it would have been a slight improvement over your usual attempts, Travis.
Do tell, Mr. Schwochert, do tell. I suspect that my library access is a tad superior to that in Endeavor, Wisconsin.
Oh, and Travoid? You and the Wikipudlians lose on IUPAC rule Lip-1.16, too. HTH. HAND. FOADIAF.
!
The carboxyl carbon is big delta (Δ), and omega (ω) is the aliphatic terminus. The reason why alpha isn't used for the carboxyl carbon is because little alpha (α) is generally reserved for naming carbons directly adjacent to carbonyl carbons (see any organic chemistry textbook). No amount of subcontinental apoplectic fury is going to make you right.
So go crawl back in your sari.
Comprehensive two-dimensional gas chromatography-mass spectrometry of complex mixtures of anaerobic bacterial metabolites of petroleum hydrocarbons
Journal of Chromatography A
C. Aitken
You're wrong Narad. The carboxyl carbon is big delta (Δ), and omega (ω) is the aliphatic terminus. The reason why alpha isn't used for the carboxyl carbon is because little alpha (α) is generally reserved for naming carbons directly adjacent to carbonyl carbons (see any organic chemistry textbook). No amount of subcontinental apoplectic fury is going to make you right.
So go crawl back in your sari.
Comprehensive two-dimensional gas chromatography-mass spectrometry of complex mixtures of anaerobic bacterial metabolites of petroleum hydrocarbons
Journal of Chromatography A
C. Aitken
Wrong. The carboxyl carbon is big delta (Δ), and omega (ω) is the aliphatic terminus. The reason why alpha isn't used for the carboxyl carbon is because little alpha (α) is generally reserved for naming carbons directly adjacent to carbonyl carbons (see any organic chemistry textbook). No amount of subcontinental apoplectic fury is going to make you right.
So go crawl back in your sari.
Comprehensive two-dimensional gas chromatography-mass spectrometry of complex mixtures of anaerobic bacterial metabolites of petroleum hydrocarbons
Journal of Chromatography A
C. Aitken
You're mind-numbingly stupid Narad. The carboxyl carbon is big delta (Δ), and omega (ω) is the aliphatic terminus. The reason why alpha isn't used for the carboxyl carbon is because little alpha (α) is generally reserved for naming carbons directly adjacent to carbonyl carbons (see any organic chemistry textbook). No amount of subcontinental apoplectic fury is going to make you right.
So go crawl back in your sari.
Comprehensive two-dimensional gas chromatography-mass spectrometry of complex mixtures of anaerobic bacterial metabolites of petroleum hydrocarbons
Journal of Chromatography A
C. Aitken
Is this publication any good? It seems to support my earlier claim that IGF-1 levels are a potential mechanism through which diet can affect cancer growth.
"Dietary and pharmacological modification of the insulin/IGF-1 system: exploiting the full repertoire against cancer"
http://www.nature.com/oncsis/journal/v5/n2/full/oncsis20162a.html?foxtr…
(don't worry Panacea, not asking you)
Unbelievable.
Wrong. The carboxyl carbon is big delta (Δ), and omega (ω) is the aliphatic terminus. The reason why alpha isn’t used for the carboxyl carbon is because little alpha (α) is generally reserved for naming carbons directly adjacent to carbonyl carbons (see any organic chemistry textbook). No amount of subcontinental apoplectic fury is going to make you right.
Review the nomenclature.
Comprehensive two-dimensional gas chromatography-mass spectrometry of complex mixtures of anaerobic bacterial metabolites of petroleum hydrocarbons
Journal of Chromatography A
C. Aitken
It is an operation. The carboxyl carbon is big delta (Δ), and omega (ω) is the aliphatic terminus. The reason why alpha isn’t used for the carboxyl carbon is because little alpha (α) is generally reserved for naming carbons directly adjacent to carbonyl carbons (see any organic chemistry textbook). No amount of subcontinental apoplectic fury is going to make you right.
Review the nomenclature.
Comprehensive two-dimensional gas chromatography-mass spectrometry of complex mixtures of anaerobic bacterial metabolites of petroleum hydrocarbons
Journal of Chromatography A
C. Aitken
No. That would have been wrong; a hyphen is not a minus sign. The minus sign sits on the same level as the plus sign and it's longer: (- − +)
Do you really need an example?
Endothelial Cell Apoptosis Induced by the Peroxisome Proliferator-activated Receptor (PPAR) Ligand 15-Deoxy-Δ12,14-prostaglandin J2
Journal of Biological Chemistry
David Bishop-Bailey
Weird how the rule you cite is in direct opposition to what you are saying, and confirms exactly what I've been trying to tell you:
That's not a style guide, Fuckleswoth, and apparently, your reading skills are abysmal.
Sigh. Another day when I was too busy and beat to provide new material and look what happened. I'm definitely going to have to make sure to step up tomorrow.
Wow, not since the days of Sheri Lewis have I seen that level of sock puppetry.
Maarten, oh, showing you how wrong you are is fun. That's easy to do when you provide the actual citations.
It's watching dumb advertising in the form of "educational video" that's the waste of time.
So with your latest link let me ask you this: just what does tinkering with how insulin works have to do with a vegan diet? How does this support your contention that a vegan diet somehow prevents or is useful in treating cancer?
Panacea, my claim is that diet (in general) may somehow prevent or be useful in treating cancer.
I gave the vegan diet as an example, based on the argumentation by Greger, which you rejected a priori (because you already know that analyzing his arguments would be a waste of time).
I offered the publication on the ketogenic diet and the publication in nature as support for my general claim.
ps I would be still interested why you object to his video. To me it's no different from attending a lecture in real life: it's just slides showing highlights from peer reviewed papers, with a voice over. Do you avoid any such presentations in general?
Orac,
Can you do me a kindness? The post #88 is not by me. Some crank has decided to start posting in my identity, as has happened elsewhere.
You can check the IP and email address to see that it isn't me.
What his or her game is, god only knows.
It's gone. It looks like our resident impersonating troll is back. I will try to be more vigilant. It sure was nice the three months or so during which he gave up.
It's probably Travis, Brian.
Good news is, I think the regulars here knew it wasn't you instantly. But yeah the fake post needs to go.
Maarten: what I rejected categorically was watching videos that were clearly advertisements. I went to Dr. Greger's website. Once I realized it is a commercial website (and it is, he's abusing his 501(c)(3) status, I realized the videos would have nothing of substance to offer any discussion.
You provided the citations for the videos as asked, and I looked at one . . . and it doesn't say what it purports to say in its own title. If Greger is using such poorly sourced material to support his claims then it merely strengthens my decision not to watch them.
Hence my "waste of time" comment.
I actually MAKE similar presentations (though likely with lower production values) as I use the flipped classroom model to teach nursing. But videos take far longer to watch than an article takes to read, and my time is valuable. Greger's videos may rely on peer reviewed research (some of which isn't very good), but that doesn't make his VIDEOS THEMSELVES peer reviewed and that's what we demand here in terms of evidence.
Certainly the hypothesis that diet may play a role in cancer prevention or treatment is interesting enough that plenty of people are doing research on it. But the results aren't conclusive, and your original claim acts as if they are.
Let me remind you that the first two things you posted on this thread were complaints about Orac's article. You didn't address the core arguments Orac made. You simply dismissed him out of hand.
So of course some of us (including me) took issue with that. Only when Orac returned the dismissal in kind did you feel stung enough to write this:
Orac (in the article): “We know that diet and certain environmental exposures can modulate cancer risk for certain cancers, but once the cancer is already established it’s too late for that.”
This is a true statement by the way, consistent with what you'll find in any medical (and nursing) textbook on the subject of cancer.
Maarten: How do you know that its not possible through diet to give the body a significantly increased change to beat an established cancer? Saying it’s not possible (or that there is no reason to assume that it could be possible) seems quite a claim.
Answer: because so far no one has ever been able to show an ability to do that. There are lots of folks who have claimed diet was the key they used to beat their cancer. But they all either had convention treatment along with the dietary changes long enough to go into remission (meaning they can't prove it was the diet, and thus it's much more likely the conventional treatment), or they're dead. Orac has written extensively on prominent examples.
Certainly there is continued interest in the impact of diet on successful cancer treatment. We may indeed find such a link. Dr. Greger acts as if we have the answer NOW, and we don't.
Pananea, my general claim was that "it could be possible that a change in diet significantly increases the bodies ability to heal itself from cancer".
In answer to Chris' question about a possible mechanism, I claimed that "diet may impact cancer growth through its relation to the IGF-1 levels in the body", and I gave some reasons (that apply in the context of the vegan diet) to back that up. I also gave reasons why I believe that Harriet Hall's critique of Greger is weak.
So how is my original claim acting [sic] as if the results are conclusive?
And why do you consider his website a commercial activity? Most succesful charities have paid staff, are they also commercial?
Isn't scientific blogging also a form of literature overview that is not peer reviewed? Is that a reason for you to avoid scientific blog posts in general? Or do you give it a chance and decide for yourself if the blogger knows what they are talking about?
Which core arguments did Orac make about my complaints about his blog? He only addressed a few words to me to tell me that I should be a little less self-righteous (he's right about that). Then he complained to you about me (I don't feel obliged to respond to comments about me but not addressed to me).
"Answer: because so far no one has ever been able to show an ability to do that." I think it would have been more accurate to say: because so far no one has ever been able to show ME an ability to do that. But if that answer (I mean the original one, that you gave) satisfies you, then indeed there is not much point for me to discuss about diet with you. OTOH if you want to discuss about other topics, such as charities, or presentation formats, then we could :-).
Yes, and the proper response to such a fantasy is can be either "so what" or "ho hum". Such a claim is indistinguishable from a claim that there's an invisible pink unicorn living in my garage, unless and until some actual, credible, empirical evidence is presented for one claim or the other. The diet fantasy is further complicated by lack of any specifics about the kind of diet or the kind of cancer.
(A strict breatharian diet would, of course, demonstrably kill a tumor, since tumors don't survive the death of the host for very long. We'll omit diets of this class.)
I'm going to skip rebutting Travis's seemingly drunken passel of repeat-posted non sequiturs, G—le scrounging, failure to check original sources, and typographic inanity unless anybody else is actually interested.
No need. I'm going to have to go back to doing what I did before and blocking each sock puppet as soon as it's identified and, even better when I can manage it, preventing him from getting new sock puppets in. Methinks a moratorium on approving new commenters might well be in order, as sad as the thought makes me. Travis sometimes sneaks by with a reasonable sounding comment before unleashing the crazy.
What kind of diseased-minded crank goes into my website, gets my anti-spam email address and uses it to pose as me in order to post at this site?
Step forward our friend from Wisconsin Dells, IP 66.206.61.192
I won't give the name now, but this is an individual with a significant personality disorder
Yeah, that's one of his IP addresses. One of many, from VPNs from varying countries all over the world. IP addresses are recorded when someone leaves a comment, and I came to recognize the most common ones used by Travis. Unfortunately, he used a lot of VPNs; so you just can't count on recognizing his IP addresses to identify him.
I'd still like a plebiscite, if anyone cares to weigh in. I could have sworn there were some chemists in this joint.
Maarten: It's possible it might rain beer some day, too? So what?
Unless you have actual evidence to back up your claims, you're just p***ing in the wind. It's not for me to produce that evidence. That's on YOU. And you haven't been able to come up with more than a "well it's possible."
Well, that's not enough.
And no, blogging is not a form of peer review. Even Orac's blog would not be considered peer reviewed because he does not submit what he writes to experts in the field before he posts.
And Orac isn't trying to create new knowledge here, which is what science does: it creates new knowledge about the natural world. What Orac does is debunk unscientific claims, or express skepticism about borderline claims using knowledge we already have. He cites sources, and he uses the scientific method and logical thinking to explain his point of view to his readers.
That makes what he has to say reliable. He doesn't pretend to always be correct, and he is open to changing his point of view when presented with new evidence . . . as are most of the regular commentors here. The key is, the evidence must be reliable itself.
It took a lot of arm twisting to get you to produce a bibliography to support your contention a bunch of videos were reliable evidence . . . and when those sources were checked, they were found to be wanting.
You haven't proved your claim, not even close. So what you say here is suspect because of that.
Ya, sure, youbetcha. Omega is always carbon 1 when omega notation is used and the carboxyl is always carbon 1 when "c" notation is used, therefore the symbol sometimes known as a hyphen effectively represents a plus sign for both those notations. Interpreting it as a minus sign would be absurd. If and only if the more meaningful n - x notation is used can it be interpreted as a minus sign, since n actually takes on a specific numeric value. But it is still the value of x, not the solution of n minus x, that is usually of interest. You can consider the symbol to be a minus sign, but that really isn't helpful if you what you want to know is how long the last dangly bit is.
Speculation:
Travis got a job and had a new group of unfortunates to try to dazzle with this all-knowing brilliance.
Travis finally annoyed the unfortunates so badly he was given the boot.
Travis returned to disgrace himself here.
Travis needs a job as a ball gag tester. Every unit subjected to stringent quality control testing!
Notably there is nothing between the omega and the nine. Might that be some sort of hint?
Of course, then you'd have to set it as one, viz., as "ω − x," like, y'know, in the original IUPAC document (PDF), where n is a number. The archived W—dia comment page puts the discombobulation in stark relief, Travis J. Schwochert's desperate G—ling for "omega minus three" notwithstanding (the lone occurrence of this in Aitken et al. also carries a conveniently omitted cite to Jarling et al.,* where it happily appears as "exclusively omega-2 and to a lesser extent omega-3 activation products are formed," with hyphens; never underestimate what bad copyediting can do).
* ht[]ps://doi.org/10.3389/fmicb.2015.00880
^ Both links work, despite my failure to properly terminate the first one.
Panacea, if you read the comment history, you will see that from the very start, I said that all claims that Greger puts forward are clearly backed by scientific references that can be easily read right off the screen of his videos. In other words, I gave you the references right off the bat, but you chose not to look at them (because that would entail watching a total of 10 minutes of video, gasp!).
Then I pointed out (on the same day) that these references are also listed directly under the video. When this was still not good enough I copy-pasted them here, all on the same day or the next day. I'm doing what I can to accomodate you, but it's never good enough.
The evidence for my more specific claim (about IGF-1) is compiled and summarized by someone you don't like, in a form that you don't like, namely: a transcript that has not been peer reviewed. In other words: it's not enough for me to present you with peer reviewed evidence, also the overview that summarizes the evidence and draws conclusions from it has to be peer reviewed to be accepted by you.
If you want to believe that you have been willing to look at the evidence, then I will leave you be in that illusion. Maybe for someone else here, the transcripts and citations lists that I posted are good enough to be the basis for a discussion, and I can discuss it with them.
ps with "to be accepted by you" I mean: to be willing to even read it.
ps 2: "He cites sources, and he uses the scientific method and logical thinking to explain his point of view to his readers."
How is that different from what Greger is doing?
ps 3: maybe if you answered my previous question, it would make your position on what presentation formats are acceptable (and which are not) more clear to me:
"I would be still interested why you object to his video. To me it’s no different from attending a lecture in real life: it’s just slides showing highlights from peer reviewed papers, with a voice over. Do you avoid any such presentations in general?"
I can't recall where it is, but something like "this paper is in the Nature family of journals is that good?"
If you had gone to the paper you would realize that
1) It is a speculative review article, not breakthrough clinical trial data
2) Almost all data about IGF-1 is in rodents that are known to be different in humans and rodents.
We never change all of human medicine because something happened in a rat.
also doesn't change that all pseudo-science appears to be well-referenced. Virtually all of the references either do not really back up the assertions (title might even sound somewhat relevant but it really is not or says the exact opposite of what the psuedoscience sales person says it does) of the person promoting the revolution to end all revolutions. Or the data is of questionable value as almost everything in all of scientific history that looks good in the test tube and the rat doesn't pan out, so no one other than the person selling the latest greatest scientific revolution to cure all things and end all death and suffering for all of time and be glorified above all others (which he or she will modestly accept even though they really want the glory more than anything) with any understanding of how science translates from the lab bench to human implementation would act upon it.
Especially because usually there is some in actual human being information that indicates it doesn't work that way.
Part of the problem with the videos is we know of the 100,000,000 just like it 100,000,009 have references that are totally meaningless.
Just because there is a reference it doesn't mean the reference in any way backs up the claim or even when it might back it up some tiny part of the claim, it is the first baby step that probably will never lead where the video dude says it can only go.
Part of peer review is you check the references to ensure it actually backs up the point being made. Sometimes they still over-sell the data, or tie together points that go beyond where you can rationally extrapolate, or cherry pick some but not all so it looks like there is no evidence that says it can't work that way, but at least if the article is peer-reviewed you might trust the long list of references a little bit. Still before making any dietary or medical changes you would want to see that it has been replicated, tested against other things, actually works in humans, etc. Ideally to the point of having systematic reviews or well-powered meta-analysis.
A few references noted in a video is just not the same, it never will be. Even if you copy them here. At least next time look up the PMID or other identifier. It helps the person reading the list find out if the are even real references (and sometimes there are errors that creep in even with the careful..there are some notable cases in the literature, especially for obscure works) and pull them up much easier if it even seems worth the time to figure out if the references really back up what they are supposed to be backing up.
Marteen, the references have to be good. They have to be right. Not all papers published in the peer reviewed literature are quality, that's why the peer review process continues after publication. Sometimes further research corrects previous research which is why the references can't be more than 5 years old (most of yours were way older than that).
You can't points to something and say "See! It has references, so it must be good."
The difference between Dr. Greger and Orac is that when Orac claims something, he's using up to date research, he doesn't cherry pick, and he actually understands what he is referencing. He isn't trying to sell the gullible a bill of goods.
Your boy picks only the references that seem to make his BS look better, which is easy when your viewers are people who don't understand science, but they hear "sciency" words coming from someone with an MD after his name so it must be "good."
And since what Greger says is what they want to hear, it's easy to believe. Real medicine and science aren't like that; it's slow, methodical and doesn't always give you the answers you expect, but it does conform to how the real world actually words.
The problem for you is, since you don't seem to understand the scientific method at all, it is very difficult for you to present any kind of an argument that will convince me, because you don't know biology, you don't know chemistry, you don't know medicine, and you don't even understand the basics of how research works or is presented.
But worse, you're not willing to learn.
Awhile back Chris asked you "I only want to see PubMed indexed studies that prove that something passing through the gastrointestinal track causes the abnormal cancer cells to stop reproducing in vivo. So no petri dish studies!"
Start there, and actually produce this, and we can start a real discussion.
KayMarie, I will ask you the same question as I have asked other people:
To me his video presentations are no different from attending a lecture in real life: it’s just slides showing highlights from peer reviewed papers, with a voice over. Do you avoid any such presentations in general?
In my opinion, a scientific talk (by an MD who devotes his career to nutrition, in this case) is a good starting point for a discussion. The talk can outline the existing evidence and make connections. It's a narrative that draws on evidence. It's not proof, but it doesn't have to be, because I am not here to proof something, but to discuss something.
Since you seem to be asking everyone, I'll give you my answer:
I avoid lectures unless:
1) They're given by someone intimately familiar with the work, like an author;
2) The lecture is a presentation of one or more related papers;
3) I've read the papers being presented;
4) The lecture includes a question-and-answer component that I can participate in;
5) Having read the papers, there still are questions in my mind that the lecturer can address.
Otherwise, the lecture is almost invariably a waste of time.
The video format necessarily misses out on one or more of these criteria, particularly when it's nothing more than a sales pitch, interpreting someone else's work.
Panacea, you refuse to attack Greger on any part of the argumentation that he puts forward (with the weak excuse that you already know it would be a waste of time to analyze it), you only attack his character and his supposed commercial intentions.
It's fine to use an older reference, as long as there is good reason to believe that the reference is still relevant for the claim that one is trying to support.
Your replies have been typical hand-waving ones, so I'm not going to spend any more effort in replying to you.
Sara, sorry, I missed your reply in the stream of other replies. Thanks for responding. I'll make sure to mind my linoleic acid intake (I used to eat a lot of pasta mixed with sunflower seed oil, and already started to substitute for rice since a few months, so I may have incidentically made the right choice).
To the other people here, sorry to have wasted your time, this blog is probably not for me. Best of luck.
ps I said I missed it but actually I failed to give it proper attention (since it was focusing more on linoleic acid than IGF-1), sorry about that. Anyway, goodbye everyone.
Maarten: "To me his video presentations are no different from attending a lecture in real life.."
In real life there is also a text book with references. Plus there is also research reports and sometime lab time to understand the material.
"In my opinion, a scientific talk (by an MD who devotes his career to nutrition, in this case) is a good starting point for a discussion."
Except during this discussion it has become clear that you do not understand the basic science. So we really are not interested in your opinion, but only the actual PubMed indexed studies to support you assertions. If you are going to assert that diet has an effect on cancer then you must produce:
"... PubMed indexed studies that prove that something passing through the gastrointestinal track causes the abnormal cancer cells to stop reproducing in vivo. So no petri dish studies!”
So where is it?
If the foundation is bad, the whole house is in bad shape.
Greger's foundation is very rocky indeed.
So if you can't defend the underlying facts, the videos are worthless. You're the one claiming they're so great. It's not up to me to take up my valuable time watching them. You need to convince me it's worth the time and effort, and you haven't.
If you're not willing to do that, then you're right. This blog might not be the place for you.
Se Habla Espol: "Since you seem to be asking everyone, I’ll give you my answer:"
There is a ScienceBasedMedicine blog entry by Dr. Harriet Hall that was posted twice. Of course Maarten did not like it. Possibly because it has this paragraph:
But, it seems Maarten does not want to be told he is being gullible.
Well, not in real papers; I haven't seen you establish this window as a criterion for the now-flounced Maarten, so I'm wondering whether that's what you meant.
It is what I meant. I alluded it to it with the discussion of the article I reviewed for him; that article was 12 years old.
I don't change my entire scientific world view or lifestyle from a single scientific lecture .
I don't know anyone that asks the audience to do that, either.
I do the same follow up for lectures I would do for any other source of scientific information.
Are the references to preliminary data in rats or test tubes or for systematic reviews of human clinical data?
Are the references selected by cherry picking for the few that seem to go that way even if there are many better and more recent papers that show that line of inquiry did not pan out.
Yes it can be a starting point, but it seems you feel that one lecture is done, deal. Since there are references it must be real, not that maybe you should actually review the references and see if they actually back up the assertions being made. And it is terrible that we question it in anyway. If no one can question it, that isn't a starting point for a conversation that leads to investigation and discovery.
If I make this into a youtube and flash references on the screen would you believe me?
Second time today I'm reading of "attacks" on people.
If I'm getting ready to take out a car from the motor pool and someone points out that I picked the one with the bad brakes, that isn't an attack.
Hitting me over the head and taking the keys away from me, that's an attack.
You're still trying to pretend that you're correct, Narad Rampersad, by writing this off as an exception?
That's so gradeschool.
You had the word "fμcklesworth" in the comment that I was quoting, so my posts were held-up in moderation. It took me a while to figure-out why.
(Orac usually clips those redundancies, but this time had decided to post them to make me look drunk.)
Hyphens are wrong. This person does it right: http://ajcn.nutrition.org/content/79/6/935.full
(And it's⇑ not a bad article. Not a bad way to familiarize yourself with eicosanoids and the carcinogenic potential of linoleic acid.)
Go away Travis Schwochert from Endeavor, Wisconsin.
Fucklesworth, you and your imaginary credentials in both chemistry and typesetting simply aren't worth the effort.
Sometimes.
^ Rats.
In one of your recent blogs about cancer treatments you referenced a web site that you used to enter details of a person's cancer diagnosis and it then output statistics to do with efficacy of surgery, surgery + chemo [ type specific ] and surgery + chemo [ type specific ] + radiation. I thought it was this blog post but can't seem to find that web site reference here. Anyone remember what recent post that was and what the web site url is?